Cerebral Palsy and Vitamin D - many studies
Cerebral Palsy is strongly associated with preterm birth
Adding Vitamin D or Magnesium or Omega-3 during pregnancy has been found to reduce preterm births
Suspect that adding all 3 early in pregnancy will greatly reduce preterm births as well as Cerebral Palsy
Cerebral Palsy: 42% are Vitamin D Deficient - meta-analysis March 2024
Prevalence of vitamin D deficiency in children with cerebral palsy: a meta-analysis
Pediatric Neurology https://doi.org/10.1016/j.pediatrneurol.2024.03.021
Kamel Awadh Alenazi , Ahmad Ayadah Alanezi
Background
Vitamin D deficiency stands out as a significant contributor to reduced bone mineral density in children diagnosed with CP. The objective of meta-analysis was to estimate the prevalence of vitamin D deficiency in children with CP.
Methods
This meta-analysis adhered to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guide. For CP children aged between 0 and 18 years with vitamin D deficiency, relevant articles were retrieved from PubMed, Scopus, ScienceDirect, and Cochrane. Following keywords were used: ‘cerebral palsy’, ‘children’, ‘childhood’, ‘vitamin D’, ‘vitamin D deficiency’, ‘prevalence’, and ‘frequency’. Newcastle-Ottawa Scale was used to assess methodological quality. Meta-analysis was performed using Stata 13.0.
Results
In total, seven articles were considered suitable for inclusion in the meta-analysis out of 411 articles initially identified. These studies involved a total of 430 children diagnosed with CP, ranging in age from 0 to 18 years. Among the seven studies, two followed a cross-sectional approach, while the remaining five utilized a case-control design. Six of these studies were determined to have a low risk of bias, while one exhibited a moderate risk of bias. The combined prevalence of vitamin D deficiency in children with CP was determined to be 42.18% (95% confidence interval [CI] = 32.90% – 51.73%, I2 = 74.41%, and P < 0.001).
Conclusions
In conclusion, this meta-analysis reveals evidence of high prevalence of vitamin D deficiency in children with CP. This finding underscores the importance of addressing nutritional factors in the management of CP among pediatric populations.
Introduction
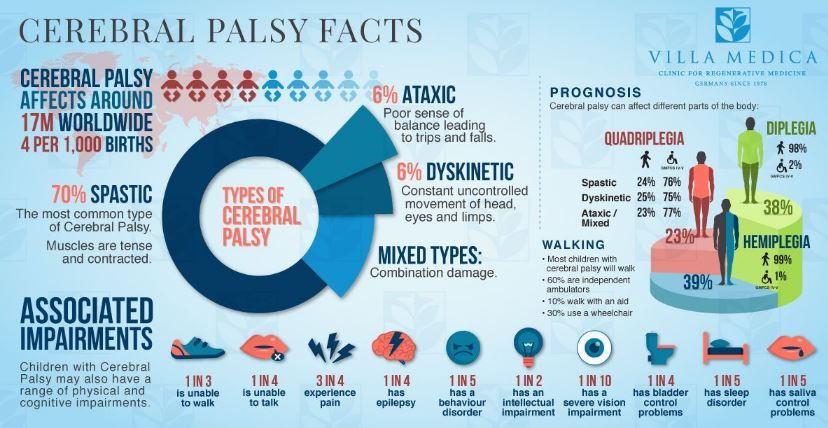
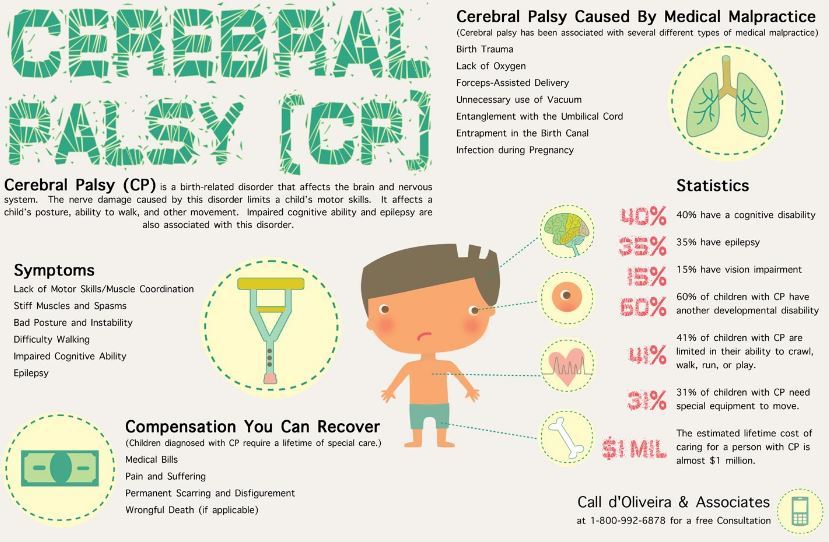
Cerebral palsy (CP) encompasses a diverse range of neurological developmental conditions that affect children, characterized by various physical signs like abnormal posture, difficulty in maintaining balance, and atypical movements. The etiology of CP is attributed to cerebral injury or dysfunction.1 Although motor impairments are often the most noticeable aspects of CP, it frequently co-occurs with sensory, musculoskeletal, perceptual, cognitive, behavioral, communication challenges, and even epilepsy.1,2 Additionally, children with CP experience a significantly diminished quality of life (drinking, eating, bathing etc) due to restricted mobility caused by unpredictable muscle tone, unsteady gait, uncontrolled movements, and poor balance.1,3
Children who have CP may have an increased risk of having lower bone mineral density due to various factors, including inadequate nutrition, insufficient vitamin D levels, limited physical activity from being non-ambulatory, diminished weight-bearing activities, the use of anti-epileptic medications, and delayed puberty.4 Vitamin D deficiency stands out as a significant contributor to reduced bone mineral density in children diagnosed with CP. These children often face challenges related to their dietary consumption of calcium and vitamin D owing to feeding difficulties. Moreover, their limited mobility often keeps them indoors with limited exposure to sunlight. Furthermore, it is worth noting that many children with CP also have epilepsy, and numerous studies have pointed to the use of anti-epileptic drugs (AEDs) as a factor that can lead to lower vitamin D levels.5, 6, 7
Vitamin D deficiency poses significant health risks, particularly in children with CP, impacting bone health and overall well-being. CP is a common neurological disorder in children, but existing studies on the prevalence of vitamin D deficiency in this population have produced variable results.1,8, 9, 10, 11, 12, 13A meta-analysis is vital to consolidate these findings, offering a more precise estimate of prevalence. This analysis is essential for informed clinical decision-making, guiding healthcare practitioners in optimizing vitamin D supplementation and monitoring strategies. Moreover, it holds potential implications for public health policies and can identify subpopulations at higher risk, thereby contributing to improved care and the well-being of children with CP.
Section snippets
PRISMA 2020 statement
This systematic review and meta-analysis adhered to the revised protocols outlined in the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 Statement.14 Supplementary file provides the PRISMA checklist as Supplementary Table 1.....
Eligibility criteria
The observational research studies were deemed eligible for this meta-analysis based on the following PECO question: The population (P) comprised of children aged between 0 and 18 years, the exposure (E) was CP, the comparison (C) was not . .....
Study selection
Overall, 411 articles were initially identified, with 39 duplicates among them. Following an initial screening that involved reviewing titles and abstracts, 357 articles were excluded, resulting in 16 articles remaining for full-text review. Ultimately, 7 articles1,8, 9, 10, 11, 12, 13 were deemed suitable for inclusion in the quantitative synthesis (meta-analysis). The primary reasons for excluding full articles were as follows: prevalence could not be determined (n = 3), epilepsy children and ....
Discussion
In this meta-analysis, we examined seven research studies that assessed the vitamin D deficiency in children with CP. The prevalence of vitamin D deficiency in children with CP remains uncertain due to the predominantly cross-sectional nature of existing research. Prevalence rates have shown substantial variation, with reports such as a study from Mexico by Zaragoza et al. 2019 indicating 29.2% deficiency,13 while Alsoda et al. (2021) found 44.0% deficiency in children with CP.8 Hariprasad et
Conclusion
In conclusion, this is the first attempt to estimate the pooled prevalence of vitamin D deficiency in children with CP. This meta-analysis reveals evidence of high prevalence of vitamin D deficiency in children with CP, emphasizing the need for proactive screening and supplementation strategies to improve their overall health and well-being. This finding underscores the importance of addressing nutritional factors in the management of CP among pediatric populations.
Children with Cerebral Palsy were 2.6X more likely to be Vitamin D deficient - July 2021
Vitamin D Status in Children on Anticonvulsant Therapy
Indian J Pediatr . 2021 Jul 28. doi: 10.1007/s12098-021-03853-y
Madhava Vijayakumar 1, Ajitha Bk 2, Biju George 3, Vijayalakshmi Bhatia 4
Objective: To assess vitamin D status of children on long-term anticonvulsants, including the less studied widely used levetiracetam, and the potential risk factors for deficiency.
Method: Children on antiepileptic drugs (cases, n = 269) were compared with controls (n = 295) for serum biochemistry, 25OHD, parathormone (PTH), sun exposure, dietary calcium, and vitamin D intake.
Results: Cases had lower serum 25OHD [median (IQR) 18.4 (11.5-24.1) ng/mL] compared to controls [20.8 (15.4-26.2] ng/mL, p < 0.001), as well as more frequent vitamin D deficiency (25OHD < 12 ng/mL, 27.1%) and insufficiency (25OHD < 20 ng/mL, 57.6%) than did controls (11.2% and 46.1%, respectively). Significantly lower median (IQR) serum calcium [8.8 (8.1-9.4) vs. 9.2 (8.5-10.0) mg/dL], phosphorous [3.8 (3.3-4.2) vs. 4.7 (4.0-5.3) mg/dL), and higher PTH [58.4 (42.9-85.8) vs. 38.9 (24.6-55.5) pg/mL, p < 0.001 for all] and proportion of elevated alkaline phosphatase (11.2% vs. 5.1%, p < 0.01) was seen in cases versus controls.
Vitamin D deficiency was present in 53.4% of children with cerebral palsy (CP) versus 19.9% in those without CP (p < 0.001). Serum 25OHD did not differ between patients on cytochrome P450 inducers versus noninducers, neither among the 3 major groups, users of carbamazepine, valproate, and levetiracetam. Logistic regression analysis showed serum 25OHD < 12 ng/mL to be independently influenced by case or control status, presence of CP, and season of sampling.
Conclusion: Vitamin D deficiency is common with anticonvulsant therapy, especially in those having CP. In Kerala, the hot, dry season from March to May is protective.
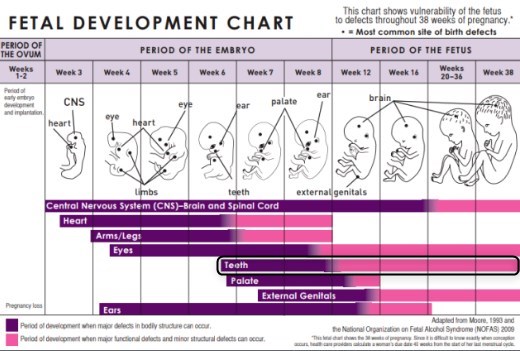
Brain development starts early, need Vitamin D, Omega-3, and Magnesium ASAP
Ensure a healthy pregnancy and baby - take Vitamin D before conception has the following
60+ items have both Cerebral Palsy and Vitamin D in the Google Scholar title (April 2025)
15 % of physically disabled children are affected by Cerebral Palsy (India)
**[Outlook India March 202
Microsoft CEO Satya Nadella’s Son, Zain, Died of CP at 26 - 2022 (he was a 36 week preemie)
](https://www.outlookindia.com/national/what-is-cerebral-palsy-disorder-that-satya-nadella-s-late-son-was-born-with-news-184750)* LinkedIn *Note Half of all premies have CP, 45X increase in CP if extreme preterm
Cerebral Palsy much worse if low vitamin D - Aug 2018* Vitamin D status of children with cerebral palsy: Should vitamin D levels be checked in children with cerebral palsy? *North Clin Istanb. 2018 Aug 8;5(4):341-347. doi: 10.14744/nci.2017.09581.
Akpinar P1.
OBJECTIVE: We aimed to investigate the vitamin D status of children with cerebral palsy (CP).
METHODS:
A total of 274 children (111 females and 163 males), aged between 1 and 19 years with CP, who came to the Physical Medicine and Rehabilitation, Pediatric Rehabilitation Outpatient Clinic between October 2013 and March 2017, were included in our study. Demographics, data concerning the details of each child's comorbidity, the Gross Motor Function Classification System (GMFCS), and Manual Ability Classification System (MACS) scores were recorded. The serum 25 hydroxy vitamin D [25(OH)D], calcium (Ca), phosphate (P), and parathormone (PTH) levels were also recorded.
RESULTS:
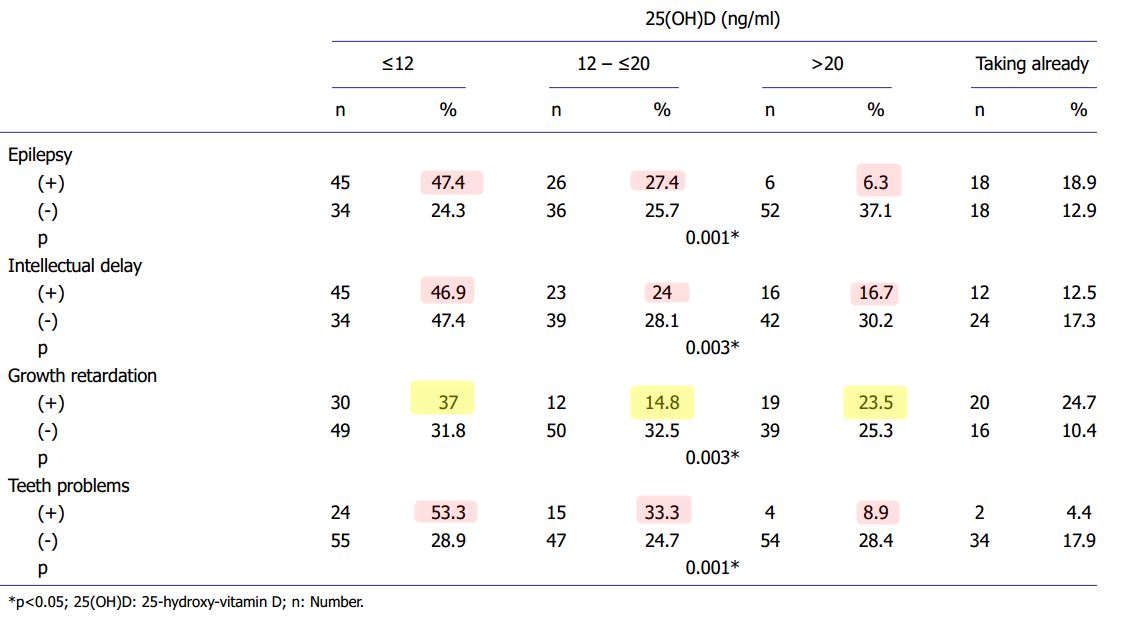
The mean age of children with CP was 7.59±6.09 years. The distribution by the CP type was 24.8% spastic unilateral, 59.8% spastic bilateral, 1.4% dyskinetic, 0.7% ataxic, 7.6% mixed, and 5.1% unclassified. The serum 25(OH)D levels of the 235 children with CP were measured. There were 79 children at the 25(OH)D level ≤12 ng/ml, regarded as vitamin D deficiency; 62 children at the 25(OH)D level 12-≤20 ng/ml, considered as vitamin D insufficiency, 43 children at the 25(OH)D level 20-≤30 ng/ml, considered as vitamin D sufficiency, and 15 children at the 25(OH)D level >30 ng/ml. A total of 36 children were already taking vitamin D supplements. There was a significant correlation between the 25(OH)D levels and GMFCS and MACS levels and associated impairments such as the epilepsy history, intellectual delay, teeth problems, and growth retardation (p<0.05).
CONCLUSION:
Our results revealed that the children with CP who are not ambulatory (GMFCS levels IV-V) and have associated impairments were prone to vitamin D deficiency, and thus should be checked for vitamin D.
{FONT(size="16")}* 📄 Download the PDF from VitaminDWiki *{FONT}
Related preterm etc in VitaminDWiki
Preterm births are VERY costly – Feb 2017
- and the costs do not appear to include the $1 million extra lifetime cost for CP
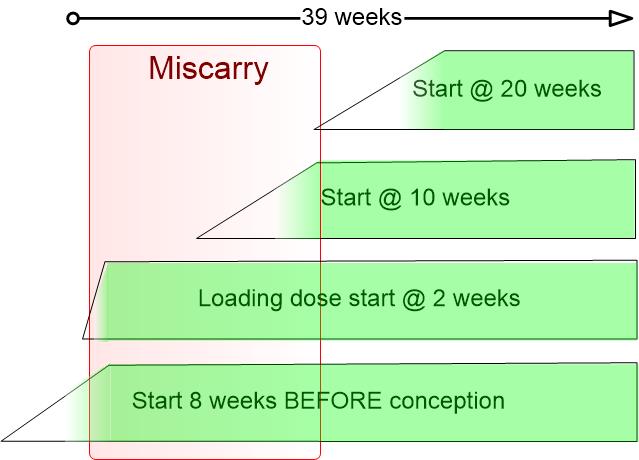
Typical pregnancy is now 39 weeks – Omega-3 and Vitamin D might restore it to full 40 weeks
Preterm birth rates increased in 15 European countries – Oct 2013
- Note: Did not notice any similar increase in CP during that time
Pre-term birth - many of risk factors are associated with low vitamin D
Preterm birth rate reduced by vitamin D – 78 percent if non-white, 39 percent if white – July 2017
Pregnancy helped by Magnesium - many studies* Cerebral palsy ** Cerebral palsy language development significantly helped by vitamin D – Sept 2015
Can you prevent Cerebral Palsy? Here’s how Vitamin D could play a powerful role in preventing CP Aug 2017
[https://my-emma.org/2017/08/16/can-you-prevent-cerebral-palsy-heres-how-vitamin-d-could-play-a-powerful-role-in-preventing-cp/|* Online *] Aug 2017
South African mother, who is a hospital doctor, gave birth prematurely and her daughter had Cerebral Palsy
She later learned about the great reduction in premature births by the efforts of Grassroots Health
Just to make the link to CP clear –* Cerebral Palsy occurs in 60% of all premature births *and is associated with intra-uterine infections of pregnancy.
If you can prevent infections and premature birth, you can very likely help prevent Cerebral Palsy.
VitaminDWiki - Many Neurological Diseases fought by Vitamin D - Dec 2022
From the Web
Vitamin D deficiency in children with cerebral palsy: A narrative review of epidemiology, contributing factors, clinical consequences and interventions - April 2022, https://doi.org/10.1016/j.sjbs.2021.12.026 FREE PDF
Vitamin D status of children with cerebral palsy: Should vitamin D levels be checked in children with cerebral palsy? - 2018 Aug 8 - doi: 10.14744/nci.2017.09581 FREE PDF
Vitamin D and iron deficiencies in children and adolescents with cerebral palsy - March 2021 https://doi.org/10.1016/j.nrleng.2017.11.005 FREE PDF* Cerebral Palsy—Trends in Epidemiology and Recent Development in Prenatal Mechanisms of Disease, Treatment, and Prevention Feb 2017 *Full free PDF online
"Overall, the total rate of CP is relatively stable, yet the contribution of prematurity and its complication to the prevalence of this syndrome are steadily increasing due to improvements in obstetric and neonatal care"
"Any intervention that will lead to modification of the risk factors for CP as well as for the prevention or treatment of the underlying mechanisms that leads to this syndrome eventually will affect its prevalence."
Cerebral Palsy >100X more likely if early preterm (note preemies have very low Vitamin D)* Cerebral Palsy Among Children Born Moderately and Late Preterm- 2014 *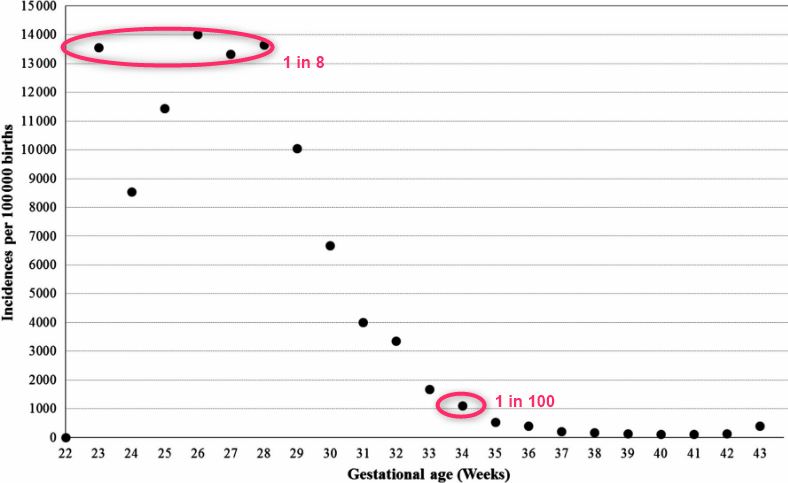
CP Risk Factors* |URL *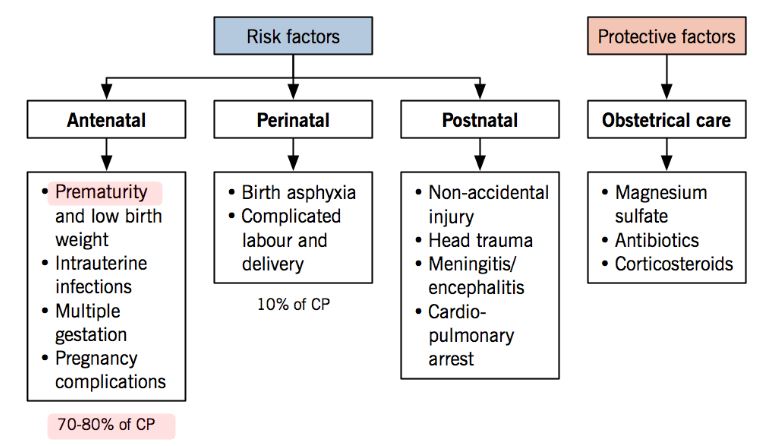
What are the risk factors for cerebral palsy?- NIH* |NIH Low birth weight or preterm birth **. Infants born preterm (defined as before 37 weeks of pregnancy) and infants who weigh less than 5.5 pounds at birth are at greater risk of cerebral palsy than are early term (defined as 37 weeks to 38 weeks of pregnancy) and full-term (defined as 39 weeks to 40 weeks of pregnancy) infants and those who are heavier at birth. The earlier the birth and the lower the infant’s birthweight, the greater the risk.
Multiple gestations. Twins, triplets, and other multiple births are at higher risk of cerebral palsy. The risk is also greater for an infant whose twin or triplet dies before or shortly after birth.
Infertility treatments. Infants born from pregnancies resulting from the use of certain infertility treatments are at higher risk for cerebral palsy than are infants born from pregnancies not related to infertility treatments. Much of this increased risk may be due to the fact that infertility treatments are more likely to result in preterm delivery and multiple gestations.
Infections during pregnancy. Toxoplasmosis, rubella (German measles), cytomegalovirus, and herpes can infect the womb and placenta, leading to brain damage in the fetus.
Fever during pregnancy. Sometimes fever in the mother during pregnancy or delivery can lead to brain damage in the fetus, resulting in cerebral palsy.
Blood factor between mother and fetus does not match. Those who have a certain protein found on red blood cells—abbreviated Rh—are Rh positive; those who do not have the protein are Rh negative. If a mother’s Rh factor is different from that of the fetus, her immune system may attack the blood cells of the fetus, including blood cells in the brain, which can lead to brain damage.
Exposure to toxic chemicals. If a mother is exposed to a toxic substance, such as high levels of methyl mercury (found in some thermometers and in some seafood), during pregnancy the fetus is at higher risk of cerebral palsy.
Maternal medical conditions:
Abnormal thyroid function
Intellectual and developmental disability
Too much protein in the urine
Seizures
Complicated labor and delivery. Infant heart or breathing problems during labor and delivery and immediately after birth increase the risk of cerebral palsy.
Jaundice (pronounced JAWN-dis). Jaundice, which causes an infant’s skin, eyes, and mouth to turn a yellowish color, can be a sign that the liver is not working normally. Jaundice occurs when a substance called bilirubin (pronounced BIL-uh-roo-bin) builds up faster than the liver can clear it from the body. This condition is common and is usually not serious. However, in cases of severe, untreated jaundice, the excess bilirubin can damage the brain and cause cerebral palsy.
Seizures. Infants who have seizures are more likely to be diagnosed with cerebral palsy later in childhood.* Some risk factors for acquired cerebral palsy are; ** Infancy. Infants are at greater risk than older children for an event that causes brain damage.
Preterm or low birthweight. Children born preterm or at a low birthweight have a higher risk for acquired cerebral palsy.
Not getting certain vaccinations. Childhood vaccinations can prevent brain infections that can cause cerebral palsy.
Injury. Not taking certain safety precautions for infants or lack of adult supervision can lead to injury that can cause cerebral palsy.
* Most of the CP risk factors are also risk factors for low vitamin D
- even twins or infertility treatments.
Observation by VitaminDWiki **---
Vitamin D in Iran CP 28 ng, other children in hospital 30 ng - 2018* Prevalence of Vitamin D Deficiency and Associated Risk Factors in Cerebral Palsy A study in North-West of Iran. *Iran J Child Neurol. 2018 Spring;12(2):25-32.
Toopchizadeh V1, Barzegar M2, Masoumi S1, Jahanjoo F1.
OBJECTIVE:
This study aimed to compare the prevalence of 25-hydroxyvitamin D deficiency in cerebral palsied (CP) with healthy control children and evaluate possible correlations between 25-hydroxyvitamin D and severity of CP and motor function.
MATERIALS & METHODS: In this case-control study, serum levels of 25-hydroxyvitamin D were evaluated in 65 children with CP and compared with 65 healthy children referred to Tabriz Pediatric Hospital, Tabriz, northwestern Iran in 2015. Blood samples were taken to measure levels of 25-hydroxyvitamin D, calcium, phosphorus and alkaline phosphatase. Regarding 25-hydroxyvitamin D levels, patients were classified as sufficient (≥30 ng/ml), insufficient (20-30 ng/ml) and deficient (<20 ng/ml).
RESULTS: Mean 25-hydroxyvitamin D levels were* 28.03±24.2 ng/ml in patients and 30±1.94 *ng/ml in control group. 25-hydroxyvitamin D deficiency was seen in 44.6% of CP and 18.5% of healthy children. There was no significant difference in 25-hydroxyvitamin D levels between boys and girls, CP types and use of antiepileptics in case group. There was significant negative correlation between age and 25-hydroxyvitamin D levels (P=0.007). The correlation between 25-hydroxyvitamin D and Gross Motor Function Classification System was not significant.
CONCLUSION: 25-hydroxyvitamin D deficiency is common in children with CP in comparison with healthy children. There was significant negative correlation between age and 25-hydroxyvitamin D levels. Routine measurement of 25-hydroxyvitamin D levels and its proper treatment is recommended to prevent its deficiency and subsequent consequences.
Cerebral Palsy supplementation with Vitamin D, some also needed Iron - Aug 2019
{FONT(size="16")}* 📄 Download the PDF from VitaminDWiki *{FONT}
Results
Patients’ mean age was 11.1 ± 4.9 years; 43 (62.3%) were male; and 56 (81.2%) had moderate-to-severe CP. Thirty-five (50.7%) used a nasogastric tube and/or gastrostomy; 15.4% were underweight and 73.8% were eutrophic, all with normal height.** Twenty (29%) and 4 patients (6.2%) received VD and iron supplementation , respectively. Albuminaemia was normal in all patients. Mean 25(OH)D level was 24.3 ± 8.8 ng/mL; 33 patients (47.8%) had insufficiency and 21 (30.4%) deficiency; 36 patients (52.2%) had low ferritin levels__. There was no association between 25(OH)D level and the other variables studied. Low ferritin levels were found to be associated with older age (P = .03), being male (P = .006), and feeding tube use (P = .006).
Conclusions
The patients studied mainly had moderate-to-severe CP, with a high frequency of suboptimal VD values and low plasma ferritin; few patients received VD and/or iron supplementation. We suggest monitoring 25(OH)D and ferritin levels due to the high rate of deficiency of these nutrients; public hospitals should be equipped with drugs to treat these deficiencies.
2+ other Cerebral Palsy studies in VitaminDWiki
The list is automatically updated
{LIST()}