Vitamin D provides many benefits and is cost-effective (need 32-40 ng) – Summer 2013
Effect of vitamin D status on pharmacological treatment efficiency: Impact on cost-effective management in medicine
Dermato-Endocrinology • Volume 5 • Issue 2
Elzbieta Karczmarewicz, * Edyta Czekuc-Kryskiewicz, Paweł Płudowski
At least 80% of the whole Polish population, including prepubertal children and adolescents, adults and seniors, are vitamin D deficient, defined as 25(OH)D < 50 nmol/L.
83% of Polish newborns start their lives at the state of vitamin D deficiency because 78% of their mothers are also deficient.
It was observed that treating patient vitamin D deficiency to vitamin D status serum 25(OH)D) 75–100 nmol/L increased effectiveness of therapies in infectious diseases (chronic hepatitis C, tuberculosis), osteoporosis, multiple sclerosis, epilepsy, Chronic Kidney Diseases and atopic dermatitis. . For these reasons doctors should take special attention to vitamin D status in patients suffering for these diseases properly implementing recent vitamin D recommendation.
PDF with references is attached at the bottom of this page
Introduction
Understanding of vitamin D role in optimal health has expanded greatly in the past few years. Grant1 indicated that increasing western Europeans’ serum 25(OH)D levels to at least 100 nmol/L all year could significantly reduce rates and economic burdens of several types of diseases whereas the reduction in healthcare expenditures was estimated to be 187,000 million Euro per year. The most important benefits would come for cancer, cardiovascular disease, diabetes mellitus, respiratory infections, dental/periodontal diseases and other. For these reasons the Polish consensus on vitamin D supplementation and standards were published on the beginning of 20102 and implemented into practice. However, data concerning epidemiology of vitamin D deficiency in Poland is still alarming. High prevalence of vitamin D deficiency has other economic burdens. It negatively affects effectiveness of expensive pharmacotherapies in infectious diseases (chronic hepatitis C, tuberculosis), osteoporosis, multiple sclerosis, epilepsy, Chronic Kidney Diseases and atopic dermatitis.
Recent studies suggest that the prevalence of vitamin D deficiency is continuously increasing worldwide.3,4 It is estimated that more than 1 billion people of all ages worldwide have serum 25(OH)D values < 75 nmol/L. The prevalence of both vitamin D deficiency [25(OH)D < 50 nmol/L] and insufficiency [50 nmol/L < 25(OH)D < 75 nmol/L] increased in 10–15 y from 22% to 33% (NHANES III 1988–1994) to 36% and 41% (NHANES 2001–2004) respectively. Recent surveys performed in Poland5-16 evidenced more frequent vitamin D deficiency in the Polish population than in the United States.
Table 1 displays prevalence of serum 25-hydroxyvitamin D (25[OH]D) level of less than 50 nmol/L in the broad ages spectrum of polish population.
It was found that in winter 83% of Polish newborns started their lives in a state of vitamin D deficiency because 78% of their mothers were also deficient. Evaluation of vitamin D status during childhood and adolescence indicated marked improvement up to the 6th month of life. From the 12th month of life (or even slightly earlier) vitamin D status gradually deteriorated. More than 80% of prepubertal and pubertal children are vitamin D deficient. At least 80% of the whole Polish population, including children and adolescents, adults and seniors, were vitamin D deficient (25(OH)D < 50nmol/L). The prevalence is much higher of vitamin D deficiency and insufficiency. In small studies from Polish hospitals more than 90% of hypertension adolescents and women with ovary cancer6,7 are vitamin D deficient. In these patients vitamin D status inversely correlate with severity6 and mortality of disease7.
Generally major determinants of vitamin D status are latitude, seasonality, skin pigmentation, clothing and use of sunscreens and also supplement use and eating vitamin D fortified foods. In Poland sunlight exposure is the primary determinant of vitamin D status5,11 because there are no vitamin D fortified foods. Recommendations of vitamin D supplementation2 are not probably properly implemented in Poland.
Effect of Vitamin D Status on Pharmacological Treatment Efficacy
Recent evidence suggests that vitamin D may impact on clinical outcomes and treatment response in some diseases. Therapeutic effects of vitamin D as adjunctive therapy to basic therapies were investigated.
Vitamin D supplementation and infectious diseases
The current body of evidence supports the view that vitamin D supplementation holds promises as risk-modifying intervention in tuberculosis (TB), influenza and viral upper respiratory illnesses.17-24 There has been a particular interest on the possible role of vitamin D supplementation as adjunctive therapy in settings of infection. A clear benefit of adjunctive vitamin D therapy in TB treatment, chronic hepatitis C (CHC) infection and acute lower respiratory infections (ALRI) was observed.17-24
Interferon (IFN)-based treatment for hepatitis C virus (HCV) infection has a therapeutic limitation and side effects, a more efficient therapeutic strategy is desired. Two small prospective randomized controlled studies showed that those patients who received vitamin D3 supplementation of 2000 IU/day, targeting a 25(OH)D level > 80 nmol/L, in addition to PEG-IFN/RBV combination therapy, had higher rates of rapid virologic response (RVR; 44% vs. 17%, p < 0.001), complete early virologic response (cEVR; 94% vs. 48%, p < 0.001) and sustained virological response SVR (86% vs. 42%; OR 2.5, 95% CI 2.0−4.9, p < 0.001) in HCV-1 and SVR (95% vs. 77%, p < 0.001) in HCV-2/3 infection compared with subjects treated with standard therapy. Moreover, recipients of vitamin D3 supplementation were less likely to relapse or non-respond to antiviral therapy. Similarly, a small retrospective study showed vitamin D3 supplementation improved SVR rate in the treatment of recurrent hepatitis C post liver transplantation (53.3% vs. 18.5%, p = 0.02) (17−19). Logistic regression analysis identified vitamin D supplement [odds ratio (OR) 3.0, 95% CI 2.0−4.9] and the serum 25(OH)D levels (< 15 or > 15 ng/mL, OR 2.2) as an independent predictor of viral response indicating that adding vitamin D3 to conventional Peg/RBV therapy significantly improved viral response.19
Lange20 reported that CYP27B1–1260 rs10877012 was an independent predictor of sustained virologic response (SVR) in patients with poor-response IL28B genotypes, but not in patients with favorable IL28B genotype. Patients with chronic hepatitis C showed a high prevalence of vitamin D defficiency [25(OH)D < 20 ng/mL] during all seasons, but 25(OH)D serum levels were not associated with treatment outcomes. This study suggested a role of 1,25-dihydroxyvitamin D [1,25(OH)2D, calcitriol] produced in macrophages s important to enhance the therapeutic efficacy of medications to treat hepatitis C. However, the serum concentration of the 1,25-dihydroxyvitamind precursor, 25(OH)D was not a suitable predictor of treatment outcome in this study because its concentration was too low.
Chronic HCV infection is associated with extra-hepatic manifestations. Recent studies have suggested an immunomodulatory role for vitamin D during HCV infection. Terrier21 investigated the association between serum vitamin D status and the presence of HCV extra-hepatic manifestations. 84 of 94 patients (89%) were vitamin D deficient or insufficient (≤ 30 ng/ml). Low 25(OH)D levels correlate with the presence of mixed cryoglobulinaemia and systemic vasculitis in chronic HCV infection. These findings suggest the potential multifaceted benefits of vitamin D supplementation in HCV-infected patients.
Low serum 25(OH)D level is associated with a high risk of developing active tuberculosis (TB). Sato22 investigated the relationships between serum 25(OH)D levels and clinical course of TB after standard therapy in hospitalized patients with TB. Confirmatory tests were performed using sputum smear and culture positivity tests for Mycobacterium tuberculosis. Drug sensitivity testing was performed for all the subjects and those not showing drug resistances for the first-line anti-TB drugs were included in the study. 38 patients were included in the study (25(OH)D levels 34.3 ± 14.8 nmol/L). In 23 patients treated with the standard frst-line 4-drug regimen serum 25(OH)D levels showed significant negative correlation with time taken to obtain 3 consecutive negative sputum smears or TB bacteria cultures and indicated that low serum 25(OH)D level was a good predictor of a prolonged clinical course in patients with active pulmonary TB. Ganmaa23 examined the effect of vitamin D supplementation on tuberculin skin test (TST) conversion. This double-blind, placebo-controlled study was conducted in 120 Mongol schoolchildren (25(OH)D < 50 nmol/L). Vitamin D supplementation (800 IU/day) for 6 mo had significant favorable effects on serum 25(OH)D concentrations and on growth in stature. A trend was seen toward fewer TST conversions in the vitamin D group.
Leis24 documented that in children < 5 y old whose vitamin D intake was less than 80 IU/kg/d were greater than 4 times more likely to have ALRI compared with children with a vitamin D intake exceeding 80 IU/kg/day (OR 4.9, CI: 1.5, 16.4). Therefore increased vitamin D supplementation could prevent bronchiolitis and pneumonia the most common reasons for hospitalization in young children.
Vitamin D supplementation as adjunctive therapy in autoimmune diseases
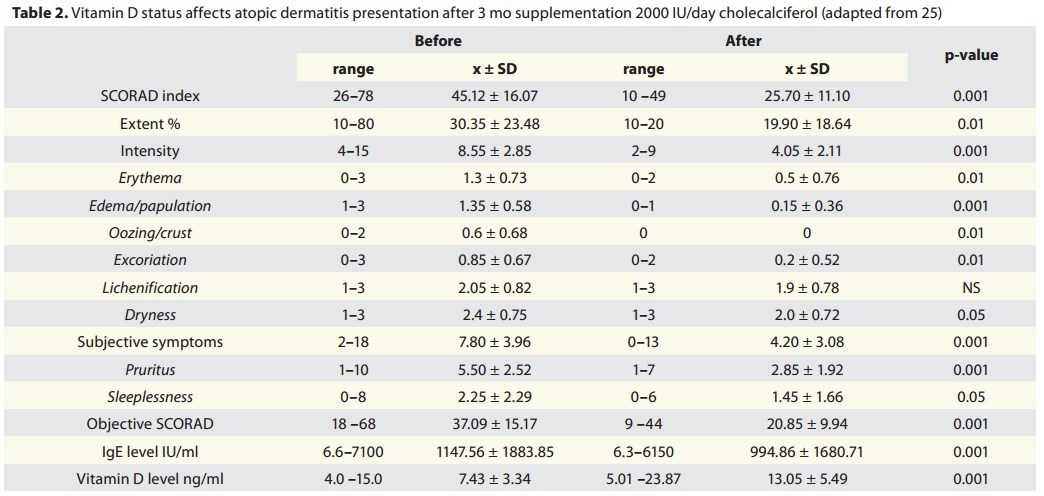
In the Polish atopic dermatitis interventional study25 vitamin D supplementation of 2000 IU/day for 3 mo in deficient patients led to 2 fold increase in 25(OH)D and 2 fold decrease in disease symptoms (Table 2).
Table 2: 2000 IU of vitamin D reduced atopic dermatitus by 2X
title by VitaminDWiki, Comment : would have been >2X if had trial had lasted longer
In Pierrot-Deseilligny observational, uncontrolled study26 vitamin D3 supplementation (3010 IU/day on average) was given to 156 patients with relapsing–remitting multiple sclerosis, under first-line immunomodulatory therapy and with initial 25(OH)D serum level lower than 100 nmol/L. Relapses were determined for 29.1 ± 8.4 and 29.8 ± 10.1 mo during and before vitamin D supplementation, respectively. It was observed that vitamin D supplementation influenced the relapse rate. Every 10 nmol increase in 25(OH)D level was associated with a reduction in the relapse incidence rate of 13.7%. According to the 25(OH)D levels, the relapse incidence rate ratio decreased as the 25(OH)D level increased up to 110 nmol/L. A plateau effect was observed beyond this limit.
Vitamin D supplementation as adjunctive therapy in CKD
Extra-renal cells, such as parathyroid cells, smooth muscle cells, endothelial cells, pancreatic cells and immunomodulatory cells, contain the machinery to locally produce 1,25(OH)2D . This may explain the associations of adequate vitamin D status with lower chronic disease risk. Thus, the ability to maintain sufficient serum concentrations of 25(OH)D, the substrate for extra-renal 1α-hydroxylase for the local production of 1,25(OH)2D, is particularly important in CKD. Shroff27 verified the hypothesis in RCT study that ergocalciferol supplementation in 47 vitamin D deficient children with CKD stages 2–4 delayed the onset of secondary hyperparathyroidism. In this randomized, double-blinded, placebo-controlled study in children with CKD2–4 who had vitamin D deficiency (median follow-up was 12 mo) the time to development of hyperparathyroidism was significantly longer with ergocalciferol treatment compared with placebo (hazard ratio, 0.30; 95% confidence interval, 0.09–0.93, p = 0.05). With ergocalciferol treatment, normal 25(OH)D levels were achieved in all 8 children with CKD2, 8 of 11 children with CKD3, but not in the single patient with CKD4. 25(OH)D levels > 100 nmol/L were required to achieve normal levels of 1,25(OH)2 D. Therefore ergocalciferol was an effective treatment that delayed the development of secondary hyperparathyroidism in children with CKD2–3. Alvarez28 documented that vitamin D3 (cholecalciferol) treatment reduced parathyroid hormone levels in 46 adult patients with early chronic kidney disease in 1 y RCT study. Subjects with early CKD (stages 2–3) were supplemented with oral vitamin D3 (vitamin D group; 50,000 IU/wk for 12 wk followed by 50,000 IU every other week for 40 wk). Serum 25(OH)D increased in the vitamin D group only [26.7 ± 6.8 to 42.8 ± 16.9 ng/mL;] and remained elevated at 1 y. PTH decreased from baseline only in the vitamin D group (baseline: 89.1 ± 49.3 to 70.1 ± 24.8 pg/mL; p = 0.01) at 12 weeks, but values were not significantly different from baseline at 1 y. Blood pressure and FGF23 did not change in either group. Thus serum PTH levels improved after vitamin D3 treatment in adult CKD patients who had secondary hyperparathyroidism.
Vitamin D supplementation as adjunctive therapy in osteoporosis
Why only some osteoporotic patients maintain a positive response to prolonged bisphosphonate therapy is unknown. Carmel29 examined bisphosphonate response and its association with serum 25(OH)D level in a “real world” setting. Serum 25(OH)D level was strongly associated with maintaining bisphosphonate response arguing that vitamin D may be involved in optimizing prolonged bisphosphonate therapy. Postmenopausal women with low bone mineral density (BMD) treated with bisphosphonates were categorized. A favorable response to biphosphonate therapy was seen in 47% patients .The definition of non-response to bisphosphonate therapy was based on the EUROFORS study, which identified patients for teriparatide therapy after “failing” anti-resorptive agents (median duration of bisphosphonate treatment was 36 mo). Non-response included any of the following: (1) T-score of < −3.0 at the lumbar spine, femoral neck, total hip or trochanter despite > 24 mo of bisphosphonates therapy, (2) decrease of > 3.0% in BMD at the lumbar spine, bilateral femoral neck, total hip or trochanter between the baseline and follow-up DEXA scans, (3) incident low-trauma fracture despite > 12 mo of bisphosphonate therapy. Patients with a mean 25(OH)D ≥ 33 ng/mL had a 4.5-fold greater odds of a favorable response. Patients with a mean 25(OH)D ≥ 33 ng/ml had a substantially greater likelihood of maintaining bisphosphonate response. The probability of inadequate response to bisphosphonate therapy measured as BMD increase was 4-fold higher in patients with 25(OH)D < 30 (OR, 4.42; 95% CI, 1.22–15.97, p = 0.02).30,31
In patients with vitamin D deficiency response to bisphosphonate therapy measured by bone turnover markers indicated that CTx decreased only by 48% in patient treated with alendronate in comparison to 61% in patient supplemented with cholecalciferol (0.266 mg/wk for 3 mo; final vitamin D status—serum 25(OH)D 82 ng/mL).32
Bertoldo33 reported that serum 25(OH)D levels modulate the acute‐phase response associated with the first nitrogen‐containing bisphosphonate infusion . Body temperature and CRP decreased when vitamin D status was normalized.
In longitudinal clinical trial (40 individuals with severe chronic periodontitis) Bashutski34 evidenced that placebo patients with baseline vitamin D deficiency [serum 25(OH)D, 16–19 ng/mL] had significantly less clinical attachment loss (CAL) gain (-0.43 mm vs. 0.92 mm, p < 0.01) and probing depth (PPD) reduction (0.43 mm vs. 1.83 mm, p < 0.01) than vitamin-D-sufficient individuals. Vitamin D deficiency at the time of periodontal surgery negatively affects treatment outcomes for up to 1 y and indicated that vitamin D status may be critical for post-surgical healing. These data are supported by work of Hokugo35 who described increased prevalence of bisphosphonate-related osteonecrosis of the jaw with vitamin D deficiency in rats. Necrotic bone in the oral cavity has recently been reported in patients treated with nitrogen-containing bisphosphonates as part of their therapeutic regimen for multiple myeloma or metastatic cancers to bone. Similar to human patients, rat ONJ lesions prolonged the oral exposure of necrotic bone sequestra and were uniquely associated with pseudoepitheliomatous hyperplasia. It was suggested that the pathophysiologic mechanism(s) underpinning ONJ may involve the interaction between bisphosphonates and compromised vitamin D functions in the realm of skeletal homeostasis and innate immunity.
The important part of osteoporosis therapy is rehabilitation after fracture. Bischoff-Ferrari36 evaluated the effect of 800–2000 IU daily cholecalciferol and extended physiotherapy (PT) on complications after hip fracture. At baseline, 50.9% of participants had 25(OH)D levels of less than 12 ng/mL and 97.7% of less than 30 ng/mL. Extended PT was successful in reducing falls but not hospital readmissions, whereas cholecalciferol treatment, 2000 IU/d, was successful in reducing hospital readmission but not falls. Thus, the 2 strategies may be useful together because they address 2 different and important complications after hip fracture.
Vitamin D supplementation as adjunctive therapy in neurological disorders
Högberg37 evidenced amelioration of depression by vitamin D supplementation in Swedish adolescents. In 54 Swedish depressed adolescents increasing mean serum 25(OH)D from 41 nmol/L at baseline to 91 nmol/L after supplementation led to decreased symptoms of depression: well-being increased (p < 0.001) and there was a significant improvement in eight of the nine items: depressed feeling (p < 0.001), irritability (p < 0.05), tiredness (p < 0.001), mood swings (p < 0.01), sleep difficulties (p < 0.01), weakness (p < 0.01), ability to concentrate (p < 0.05) and pain (p < 0.05).Vitamin D supplementation alone has therapeutic effect in vitamin D deficient depressed patients.
Huang38 described patients with multiple areas of chronic pain and supplemented with vitamin D3 1200 IU daily (if serum 25(OH)D was 20 to 29 ng/mL) or 50,000 IU weekly (if serum 25(OH)D was < 20 ng/mL) improved their pain levels, sleep and various aspects of QoL.
Khoraminya39 reported therapeutic effects of vitamin D3 (1500 IU/day) as adjunctive therapy to fluoxetine (20mg) in 42 patients with major depressive disorder. In the 8-weeks, double-blind, randomized, placebo-controlled trial depression severity based on Hamilton Depression Rating Scale HDRS and Beck Depression Inventory BDI decreased significantly after intervention, with a significant difference between the two groups—the vitamin D + fluoxetine combination was significantly better than fluoxetine alone from the 4th week of treatment.
The exact mechanism by which vitamin D exerts its beneficial effect in epilepsy is still to be explored. Vitamin D receptors as well as the 1α-hydroxylase, the enzyme that produces 1,25(OH)2D, are distributed widely in the brain.40 Vitamin D deficiency is known to be highly prevalent among epilepsy patients, but only one study, published nearly 40 y ago, documented that administration of vitamin D2 resulted in a seizure reduction of 30% on average.41 In small study of Hollo42 vitamin D3 supplementation (oral dose of 40,000–200,000 IU bolus in order to normalize vitamin D deficiency and then a daily maintenance dose of 2000–2600 IU) results in improved seizure control in patients with pharmacoresistant epilepsy. Ten (of 13) patients showed decreased seizure numbers during the 90 d following treatment onset as compared with the baseline period. Among all patients, the median seizure reduction was 40%, and there was a non-significant tendency for patients with larger proportional elevation of 25(OH)D levels exhibiting a larger proportional reduction in seizure numbers. Median serum 25(OH)D level at baseline was 11.8 ng/mL (range: 4.0–34.2 ng/mL) and rose close to the normal range in all patients (median: 38.0 ng/mL, range: 23.3–45.0 ng/mL).
Conclusions
There is a substantial and growing body of evidence indicating that the lower end of the adequate range is at least 80 nmol/L and, by some criteria, 100 nmol/L. .It was evidenced that transfering patients from vitamin D deficiency to proper vitamin D status (75−100 nmol/L serum 25(OH)D) increase effectiveness of therapies in infectious diseases (chronic hepatitis C, tuberculosis), osteoporosis, multiple sclerosis, epilepsy, Chronic Kidney Diseases and atopic dermatitis. For these reasons doctors should take special attention to vitamin D status in patients suffering for these diseases properly implementing recent vitamin D recommendation.43