Transdermal Magnesium Chloride spray - variable responses, removed toxic metals - 2010
A pilot study to determine the impact of transdermal magnesium treatment on serum levels and whole body CaMg ratios
Nurse Practioner Spring 2010
Watkins K, Josling PD*
Mineral Check, Lenham Heath, United Kingdom, **Herbal Research Centre, Battle, United Kingdom.
📄 Download the PDF from VitaminDWiki.
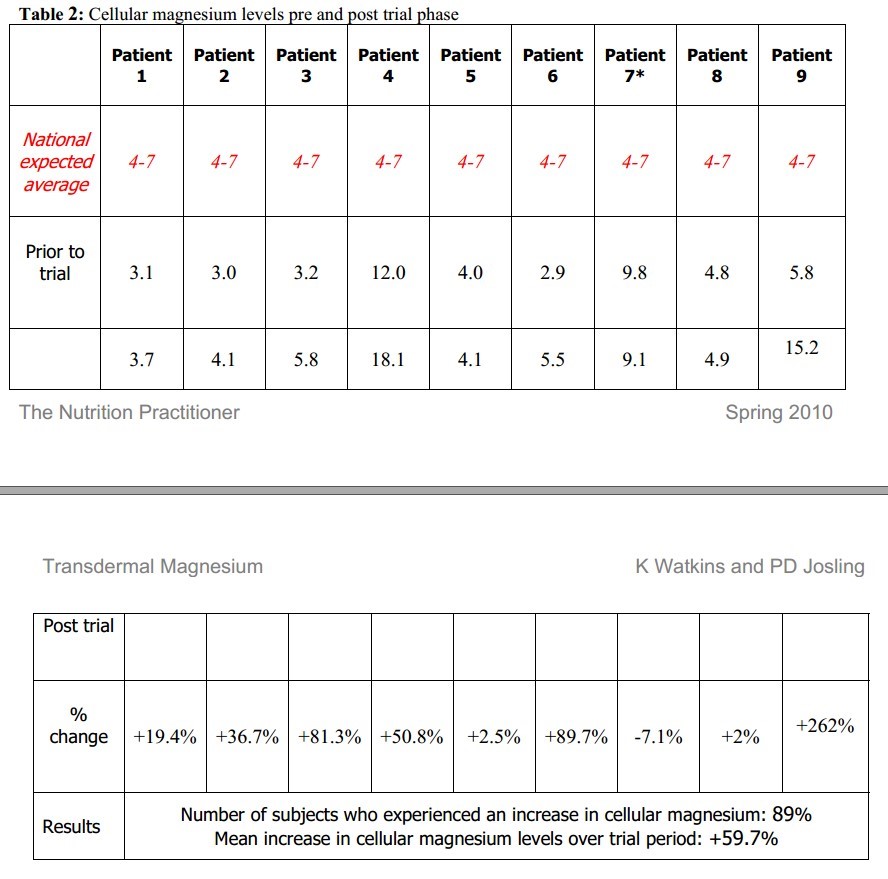
This study was designed to test whether transdermal application of a 3i% magnesium chloride formulation could alter serum magnesium levels and whole body caicium/magnesium ratios. Patients were screened using a sophisticated hair analysis to determine pre-treatment levels of cellular magnesium and then again following the adopted protocol for product application. After 12 weeks ’ treatment 89% of subjects raised their cellular magnesium levels with an average increase of 59.7%recorded. Equivalent results using oral supplementation have been reported over 9-24 months. Furthermore all patients showed an improvement in the caicium/magnesium balance ratio where the mean improvement seen over the trial period was 25.2%. Further observations indicated that 78% of patients also showed significant evidence of detoxification of heavy metais following treatment with BetterYou™ Magnesium OH. These results show that non seif selected patients who exhibit variable levels of intracellular magnesium can improve this significantly and could therefore impact on many areas of general health and well being, including cardiovascular and skeletal fitness.
Introduction
The magnesium source used for the trial was BetterYou™ Magnesium Oil Original spray and BetterYou™ Magnesium Oil Original Soak. Both contain a saturated solution of 31% magnesium chloride mined from the Zechstein sea deposits in Northern Holland. Magnesium is required as a cofactor for many enzyme systems. It is necessary for protein synthesis and for both anaerobic and aerobic energy generation through glycolysis, either indirectly as a part of magnesium-ATP complex, or directly as an enzyme activator. Magnesium plays a multifunctional role in cell metabolism and has a critical role in cell division. As well as regulating the movement of potassium in myocardial cells it is also known to act as a calcium channel blocker. Magnesium deficiency has been linked to cardiovascular, skeletal and central nervous system disorders and is essential for the normal function of the parathyroid gland and for vitamin D metabolism.
Magnesium depletion markedly disturbs calcium homeostasis, and hypocalcaemia is a common manifestation of moderate to severe magnesium deficiency. Now more than ever we need to understand that many of the degenerative diseases plaguing Western society are as a result of the mineral imbalance within our diet1 Animal and human data suggest that magnesium may play an important role in ischaemic heart disease. Few prospective epidemiological studies have related serum magnesium concentrations to mortality from ischaemic heart disease (IHD) or all-causes. However data from the National Health and Nutrition Examination Survey Epidemiologic Follow up Study showed that serum magnesium concentrations were inversely associated with mortality from IHD and all-cause mortality. It is reported that 12000 people followed for 19 years indicated that those with the highest magnesium levels had a 30% lower risk of heart disease.2
Research also shows that between 68% and 75% of individuals in the United States do not consume the daily recommended amount of dietary magnesium, and 19% of Americans do not consume even half of the government’s recommended daily intake of magnesium3. Since 1940 the magnesium content within 72 basic foods has dropped by 21 % and this situation is mimicked across several continents. Though worrying in terms of the health status of a population, the reality however is much worse. These statistics are based on a Recommended Daily Allowance (RDA) which is believed by many medical professionals to be set too low. Recently, the Independent Vitamin Safety Review Panel, consisting of academics and researchers, recommended that the RDA for magnesium should be raised because current standards are simply not adequate to prevent illnesses. In 2011 the RDA guideline for magnesium will be raised from 300 to 360mg.
Magnesium is needed for more than 325 biochemical reactions in the body. It helps to maintain normal muscle and nerve function, keeps heart rhythm steady, and is important for bone health too. As magnesium is consistently ignored in artificial fertiliser production, it is expected that many decades will pass before the soil reabsorbs this vital mineral even if we start adding it today. Whilst food fortification or oral supplementation is possible the whole process is rather slow and successful remineralisation not guaranteed to succeed3. Oral magnesium presents unique challenges for many individuals to effectively restore intracellular magnesium levels. Usage of poorly ionized forms of magnesium could be one factor to blame. Work has shown that magnesium oxide, an inexpensive magnesium complex included in popular dietary supplements could have fractional absorption in the gut as small as 4 percent. If one was to ingest the commonly recommended (albeit modest) adult dosage of 300-400mg elemental magnesium per day, this would equate to a usable dosage of only 1216mg. Even magnesium citrate, a relatively well absorbed magnesium compound, will provide a fractional absorption rate of 50% at most. And yet, realistic absorption rates from oral magnesium supplements are rarely taken into account when dosage recommendations are given.
Inconsistencies in bioavailability from one form of magnesium to the next remains a concern, but nearly all magnesium supplements share a common tendency to create a laxative effect in the bowels. The effect of different magnesium compounds on bowel motility and stool softness is further amplified with the quantity ingested in a single dose. The higher any single dosage, the greater the potential to cause diarrhoea, thereby reducing transit time through the bowels. There is reliable evidence to indicate that absorption relies heavily on magnesium’s staying power in the intestine - at minimum 12 hours. If transit time is reduced to less than 12 hours, the percentage of magnesium absorbed may be drastically impaired.
When these points of consideration are taken in conjunction with the unpredictability of each individual’s ability to absorb magnesium through oral means, the results become unreliable in many cases. In contrast, bypassing the digestive system with topical use of magnesium chloride circumvents the many common drawbacks which would accompany oral supplementation. A sensible alternative therefore is transdermal application of magnesium as the chloride salt, which offers a simple, cost effective and efficient methodology to increase both cellular magnesium levels and to adjust the balance with calcium in a positive manner. Transdermal application is the ultimate way to replenish cellular magnesium levels since every cell in the body bathes and feeds in it and even dehydroepiandrosterone (DHEA) levels may be increased naturally.4
Methodology
This trial took place over a 12 week period and involved a total of 9 patients aged between 22 and 69 years (see patient demographic in Table 1). Following provision of a hair sample for analysis of mineral content each patient tested was instructed to apply 20 sprays of BetterYou™ Magnesium Oil Original spray daily , anywhere on the body, plus a 20 minute foot soak using 100ml BetterYou™ Magnesium Oil Original Soak (using a simple water footbath) twice weekly. At the end of 12 weeks’ treatment a further hair analysis was conducted.
Table 1: Patient demographics on study entry
Mineral measurements
Hair analysis was used to measure the cellular levels of magnesium. Conventional blood tests for patients to determine a magnesium deficiency was considered but rejected as a method of analysis as blood tests determine the concentration found in blood and not what is found between the body cells. The blood and serum contain minerals but they may not be completely representative of the body’s mineral storage6. In many cases, the serum level of minerals are maintained at the expense of the tissue concentration. Serum concentrations fluctuate and excess accumulation of minerals is often undetected in the serum due to their removal from the blood for deposition into the tissues. Of the magnesium that is present within the body at any one time, only 1% is found in the blood. The rest is held within bones, muscle and tissue cells elsewhere around the body. The human body’s homeostatic mechanisms mean that blood tends to be a poor diagnostic for magnesium levels.5
Hair analysis
Hair mineral analysis (HMA) is an established technique and laboratory procedure, and most importantly research to support findings are highly reliable6. Hair is a very metabolically active tissue and as it forms, provides a permanent record of activity occurring within the body during its period of growth. The first 3 to 4 cm closest to the scalp can give a good indication of the nutritional and toxic mineral exposure over the previous six to eight weeks. Hair analysis is routinely used in occupational7, environmental and natural healthcare as a method of investigation to assist screening and/or diagnosis. HMA is an analytical test that assays the mineral composition of the hair. As a screening test, it is able to provide indications of imbalances, deficiencies and excesses of many essential and toxic minerals and can provide a comprehensive picture upon which to base the most effective nutritional therapy. For this study, it enabled the researchers to look at the presupplementation levels of magnesium (and other minerals) and to compare them post supplementation.
All analyses were undertaken by Mineral Check Limited. The laboratory uses ICP (inductively coupled plasma mass spectrometry) to test the mineral content of hair. It is a valuable screening tool as during the growth phase, metabolic activity exposes the hair to the internal environment. As the hair reaches the surface of the skin, its outer layers harden, locking in the metabolic products accumulated during this period of hair formation. The laboratory test requires 150 milligrams (approximately a teaspoonful) of hair and, by testing the 2 - 3 centimetres closest to the scalp, the test results give an indication of the metabolic environment in the previous couple of months. The laboratory is able to routinely test for 29 minerals and 9 toxic minerals , and, although initially, the research was only looking at magnesium levels, a full test was conducted to allow the researchers to look beyond just the magnesium levels.
Hair is a useful medium for testing, it is hygienic, painless to sample and has an easy storage protocol.
Whilst the laboratory test is a hair test, research shows us that hair mineral levels reflect mineral levels in other body tissues.8
All mineral measurements are recorded as milligrams percent (milligrams per one hundred grams of hair). One mg% is equal to ten parts per million (pap) of the mineral. The nine subjects were tested for cellular mineral levels via hair analysis before the trial commenced. Hair was collected under required ‘clean’ conditions and no mineral related products were allowed to be used during the trial. Analysis was then taken at the end of the trial 12 weeks later. This took place between July and October 2009.
Transdermal application
Traditional methods of administering medicine such as tablets or capsules have to pass through the stomach and unfortunately the action of stomach acids and digestive enzymes often reduces uptake and bioavailability so significantly that very little may actually reach the bloodstream. Bypassing the stomach and liver means a much greater percentage of the active ingredient goes straight into the bloodstream where it’s needed. In many cases, transdermal methods are used to help avoid potential side effects such as stomach upset or drowsiness.9 The full potential for transdermal medicine has not been utilised to any great extent by modern allopathic medicine though it has been practiced for thousands of years in hot springs around the world. It has been reported that the traditional method of introducing magnesium to the body through oral supplements is substantially less effective than the transdermal route10, but plays an even more critical role in applications to soft tissue. Transdermal delivery allows for the liver and stomach to be bypassed, which translates into a much greater percentage of the active ingredient reaching the bloodstream, and more specifically to the site of application.
Results
Mineral analysis pre-treatment indicated that 7 of the 9 patients enrolled had low cellular magnesium levels as predicted by our epidemiological analysis. After transdermal applications for 12 weeks all patients except one had a significant increase in cellular magnesium ranging from 2% to 262%. One patient ceased application prematurely, three weeks before final analysis. Overall an average increase of 59.7% was seen. See Table 2.
Table 2: Cellular magnesium levels pre and post trial phase
Personal problems forced this subject to cease transdermal magnesium application 3 weeks early The data set was then used to calculate the effect on the calcium/magnesium ratio. Based upon the ratio of calcium to magnesium within the body recommendations by nutritional practitioners can vary from a 4:1 - 1:1 (Ca/Mg) ratio. It is understood that calcium and magnesium oppose each other at the intracellular level and that calcium requires the presence of sufficient magnesium for it to become soluble within the body. Thus low magnesium intake will produce evidence of high calcium storage outside of the bone (referred to as calcification). These results are presented in Table 3.
Overall 100% of patients improved their calcium/magnesium ratio and the average improvement over the period of this study was 25.2%.
Table 3: Effect on calcium/magnesium ratio
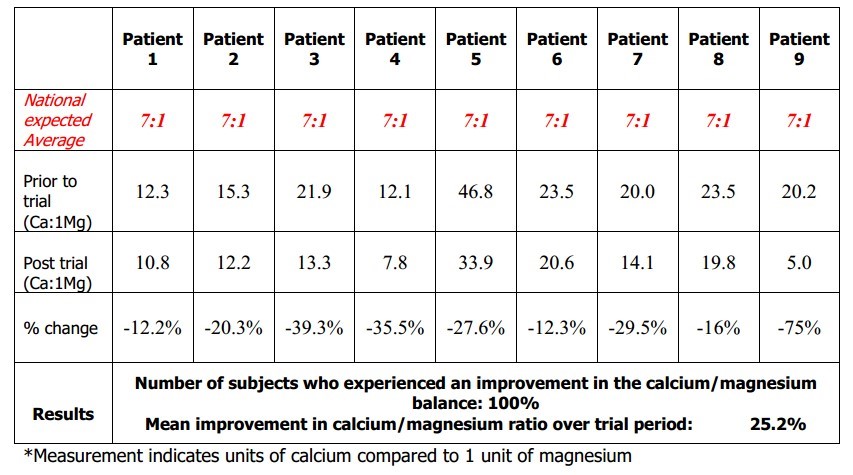
Number of subjects who experienced an improvement in the calcium/magnesium
balance: 100%
Mean improvement in calcium/magnesium ratio over trial period: 25.2%
Measurement indicates units of calcium compared to 1 unit of magnesium
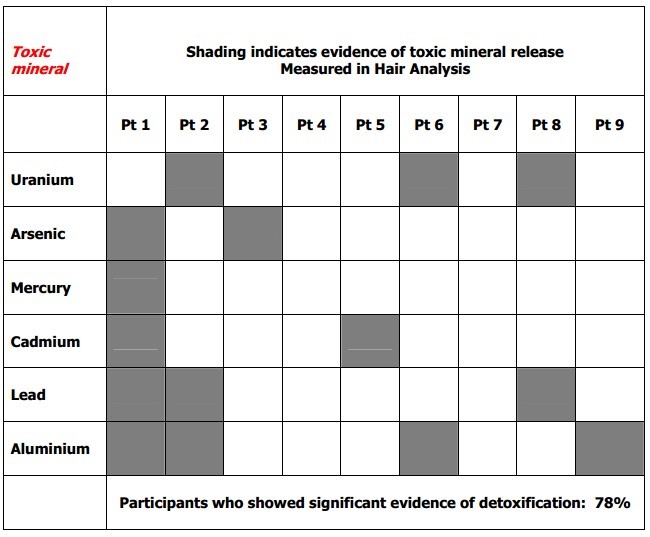
Finally, and the most surprising finding, was the effect of the magnesium on the detoxification of toxic minerals. Seven of the nine test cases, so 78%, showed that using the magnesium oil body spray alongside the foot soak was able to antagonise and release toxic minerals including aluminium, lead, cadmium and mercury amongst others. These observations are recorded in Table 4.
There are two basic relationships that exist between nutrients. In some instances they work together, or in co-operation with each other so have a synergistic relationship. At other times nutrients can work against each other in an antagonistic relationship. Antagonism of nutrients can occur at the intestinal or cellular level and the antagonistic effects of magnesium may be used by health professionals to assist detoxification at a cellular level. This research was conducted over twelve weeks and so levels during this period are likely to rise. As the toxic minerals are antagonised and so released from storage sites within the body, the level of a circulating toxic mineral may rise on a HMA prior to expulsion.
Magnesium is a well recorded antagonist for these toxic minerals but generally health practitioners will use extensive detoxification protocols with their patients/clients and yet this study showed that using a simple application of 20 daily body sprays and a twice weekly foot soak brought about some significant changes in the toxic mineral picture with minerals clearly being released from storage and excreted.
Table 4 : Effect on toxic mineral expulsion - Magnesium aids the cell’s ability to expel toxic minerals
Discussion
This pilot study represents a major step forward in both our understanding of the superior absorption qualities of the Zechstein magnesium source and also in providing evidence of the dramatic impact the mineral has on the body. Despite the relatively small sample size the results are significant. Data shows that around 74% of the population in general are likely to have sub optimal levels of magnesium and that this imbalance is unlikely to be improved by Government intervention in agricultural practices. It is clear that the concentrated chloride form of the Zechstein seabed mineral solution (Better You Magnesium Oil) can significantly improve cellular magnesium in 59.7% of these patients. The therapeutic value of magnesium chloride as a transdermal application reaches well beyond the potential of dietary magnesium as it effectively saturates the tissues, delivering high concentrations of magnesium to where it is needed most i.e. at the cellular level, directly into the circulation, entering the tissue cells immediately.
This study confirms that transdermal application of magnesium in the chloride form will raise magnesium levels within the body over a relatively short period of time. Additionally, the relationship between calcium and magnesium is important for many health aspects (for example bone building) and raising magnesium levels has a beneficial effect on the body ratio between calcium and magnesium. Again this study clearly demonstrated a beneficial effect in preventing calcium build up in body tissues meaning that the calcium could be correctly utilised. The results indicate that it is possible to increase cellular magnesium using a simple but effective transdermal compound (Better You™ Magnesium Oil) which offers convenience, efficacy and long term improvement in the critical calcium/magnesium balance that has become so difficult to achieve in today’s modern environment.
References
Expert Group on Vitamins and Minerals 2003 ISBN 1-904026-11-7
McCance and Widdowson (1940) The Chemical Composition of Foods, 1st Edition, Special Report Series No: 235, Published by Medical Research Council.
ES Ford Serum magnesium and ischaemic heart disease: findings from a national sample of US adults Int. J. Epidemiol. 28: 645-651
Niculescu T, Dumitru R, Botha V, Alexandrescu R, Manolescu N.Relationship between the lead concentration in hair and occupational exposure. Br J Ind Med. 1983 Feb;40(1):67-70.
Watts DL Trace Elements and other Essential Nutrients 1995 B-L-O-C-K.
Bass DA, Hickok D, Quig D, Urek K.Trace element analysis in hair: factors determining accuracy, precision, and reliability - Statistical Data Included. Altern Med Review 2001;6(5):472-481.
Sircus M, Transdermal Magnesium Therapy, ISBN 0-9787991-1-9, Phaelos Books.
Hopps, H. C.: The Biological Bases for Using Hair and Nail for Analysis of Trace Elements. Trace Substances In Environmental Health VIII. Hemphill, D.D., ed. University of Missouri, Columbia. 1974
Federal Drug Administration 358C38305 Administration through the dermal layer of the skin to the systemic circulation by diffusion.
Shealy, N Holy Water, Sacred Oil; the Fountain of Youth: Alibris United Kingdom.
Study was cited 17 times as of Nov 2022
Myth or Reality—Transdermal Magnesium? - Nutrients 2017, 9(8), 813; https://doi.org/10.3390/nu9080813 FREE PDF
Transdermal Magnesium - Book
Effects of transdermal magnesium chloride on quality of life for patients with fibromyalgia: a feasibility study - Sept 2015 https://doi.org/10.1016/S2095-4964(15)60195-9