Non-alcoholic Fatty Liver Disease (4 in 10 seniors) and Vitamin D
FACT: NAFLD (Non-alcoholic Fatty Liver Disease) is very common and hard to diagnose
FACT: NAFLD is associated with somewhat lower levels of vitamin D
FACT: People with NASH (a more severe form of NAFLD) do not produce as much semi-activated vitamin D
OBSERVATION: Loading doses of vitamin D help sub sequent NAFLD maintenance doses
Assumption: Livers of people with NAFLD are not able to process normal Vitamin D as well
Assumption: Other forms of Vitamin D could treat NAFLD much better than normal vitamin D
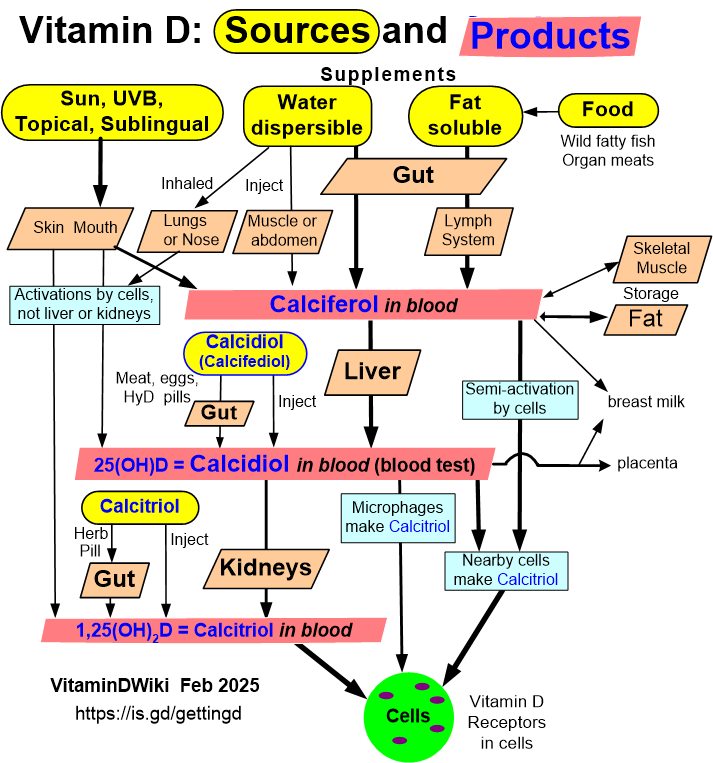
- Nanoemulsion, Bioemulsion, Calcidiol, topical
Getting Vitamin D into your blood and cells has the following chart
See VitaminDWiki
Liver associations with vitamin D and genes – Overview April 2018
Vitamin D reduces fatty liver problems in rats fed a high fat diet – June 2018
Vitamin C reduces liver inflammation, which improves vitamin D production – Dec 2014
Sleep Apnea is strongly associated with Fatty Liver Disease PDF is attached at the bottom of this page
Half of obese children had fatty liver and low vitamin D – March 2014
Hepatitis C, non-alcoholic fatty liver disease and vitamin D deficiency – Dec 2014 great summary tables
Increasing vitamin D level in blood failed to decrease Fatty Liver inflammation – RCT Aug 2014
Glyphosate Is Causing Fatty Liver Disease and many other problems - May 2019
VitaminDWiki pages with NON-ALCOHOLIC or NAFLD in title (22 as of April 2022)
This list is automatcially updated
{LIST()}
Items in both categories Liver and Vitamin D Receptor
{category}
Items in both categories Liver and Omega-3
{category}
Review Article: Non-alcoholic Fatty Liver Disease and Osteoporosis (40% of seniors) - 2012
Y. Yilmaz
Alimentary Pharmacology & Therapeutics. 2012;36(4):345-352. © 2012
Background Low bone mineral density (BMD) has been reported in both paediatric and adult patients with non-alcoholic fatty liver disease (NAFLD).
The mechanisms behind the reduced BMD in NAFLD are still not completely understood.
Aim To provide a critical overview of the pathophysiological pathways linking NAFLD, reduced BMD and osteoporosis, with a special focus on the alterations of soluble mediators which could link fat accumulation in the liver with bone health. The MEDLINE database was searched by a combination of keywords: non-alcoholic fatty liver disease OR hepatic steatosis OR metabolic syndrome OR insulin resistance AND bone mineral density OR osteoporosis OR bone AND biomarkers OR serum marker.
Results Several factors that may influence bone mineralisation and the increased risk of osteoporosis in NAFLD can be discussed. These include the release of cytokines from the inflamed liver which may influence the bone microenvironment, vitamin D deficiency, and limited physical activity. Circulating markers of bone metabolism, including osteopontin, osteoprotegerin, osteocalcin and fetuin-A, have been found to be altered in patients with NAFLD.
Conclusion A better understanding of the mechanisms that link bone metabolism and the liver may open a new frontier to fight two highly prevalent conditions like NAFLD and osteoporosis.
Introduction
The term non-alcoholic fatty liver disease (NAFLD) refers to any fatty infiltration of the liver that is not caused by significant alcohol abuse.[1–8] From an epidemiological standpoint, the prevalence of NAFLD is twice as high in men than in women (42% vs. 24% respectively), but – similar to that of osteoporosis – increases significantly among postmenopausal women.[6] In addition, in accordance with the observed epidemiological figures for osteoporosis,
the prevalence of NAFLD increases with age,
from less than 20% in people under the age of 20
to more than 40% in people aged >60 years or higher.[6]
The metabolic syndrome (MS) is universally considered as the key factor in the pathogenesis of NAFLD.[9, 10] Interestingly, low bone mineral density (BMD) has been recognised as a potential health problem in both men and women suffering from the MS,[11–14] of which NAFLD is the hepatic manifestation.[9] Moreover, preliminary evidence seems to suggest that NAFLD may be associated with an increased risk of osteoporotic fractures.[15] Although the mechanisms behind the reduced BMD in NAFLD are still not completely understood, several factors that may influence bone health and mineralisation in NAFLD can be discussed. These include the chronic low-grade inflammation itself, which causes the release of cytokines from the inflamed liver, vitamin D deficiency, and limited physical activity. Circulating markers of bone metabolism, including osteopontin, osteoprotegerin, osteocalcin and fetuin-A, have been found to be altered in patients with NAFLD.
In the present review, we provide a critical overview of the potential pathways linking NAFLD with a reduced BMD, with a special focus on biochemical alterations of circulating bone-regulating markers.
Toward this aim, the MEDLINE database was searched by a combination of keywords:
non-alcoholic fatty liver disease
OR hepatic steatosis
OR metabolic syndrome
OR insulin resistance
AND bone mineral density
OR osteoporosis
OR bone
AND biomarkers
OR serum marker.
A better understanding of the mechanisms that link bone metabolism and the liver may open a new frontier to fight two highly prevalent conditions like NAFLD and osteoporosis.
The entire article is in the PDF at the bottom of this page
85% correct predicition of fatty liver by computing ratio of ALT /AST, not need CT scan or liver biopsy - Aug 2016
ALT = alanine aminotransferase
AST = aspartate aminotransferase
Spleen may also be involved with Fatty Liver Disease - via vitamin D
Spleen: A new role for an old player? Sept 2011
PDF is attached at the bottom of this page
Prevalence and risk factors of non-alcoholic fatty liver disease in the elderly: results from the Rotterdam study.
J Hepatol. 2012 Dec;57(6):1305-11. doi: 10.1016/j.jhep.2012.07.028. Epub 2012 Aug 4.
Koehler EM, Schouten JN, Hansen BE, van Rooij FJ, Hofman A, Stricker BH, Janssen HL.
Dept. of Gastroenterology and Hepatology, Erasmus MC University Hospital, Rotterdam, The Netherlands.
BACKGROUND; AIMS: The prevalence of non-alcoholic fatty liver disease (NAFLD) appears to increase with age.
However, limited data are available concerning the prevalence of NAFLD in the elderly. Our aim was to determine the prevalence and risk factors of NAFLD in an elderly population.
METHODS: This study was based on participants in the population-based Rotterdam Study. Each participant was interviewed and had a clinical examination at the research center, including a fasting blood collection, liver ultrasonography, and anthropometric assessment. Ordinal and logistic regression analysis was used to assess associations between covariables and (severity of) NAFLD.
RESULTS: Data from 2811 participants (mean age 76.4 ± 6.0 years) were analyzed.
The prevalence of NAFLD was 35.1%.
The prevalence of NAFLD decreased with advancing age (p<0.001).
In logistic regression analysis,
age (OR 0.97; 95% CI 0.95-0.99; p<0.001),
total physical activity level (OR 0.98, 95% CI 0.96-0.99; p=0.005),
pack years of smoking (OR 1.01, 95% CI 1.00-1.01; p=0.02),
waist circumference >88 cm for women and > 102 cm for men (OR 4.89; CI 4.00-5.96; p<0.001),
fasting glucose ≥ 100 mg/dl or drug treatment for elevated blood glucose (OR 2.11, 95% CI 1.72-2.59; p<0.001),
blood pressure ≥ 130/85 mmHg or drug treatment for elevated blood pressure (OR 1.80, 95% CI 1.08-3.01; p=0.03), and
triglycerides ≥ 150 mg/dl or treatment with serum lipid reducing agents (OR 1.56, 95% CI 1.28-1.91; p<0.001)
were associated with NAFLD.
CONCLUSIONS: NAFLD is common in the elderly, although the prevalence decreases with advancing age.
Further studies are warranted exploring potential factors contributing to this apparent positive selection effect in the elderly.
Copyright © 2012 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. PMID: 22871499
Fatty Liver Disease Rises Among Heaviest Teens May 2012
- more than doubled in the past two decades, from 3.6 % to 9.9 %, outpacing the rise in teenage obesity
Diabetics with (NAFLD) not helped by weekly 50,000 Vitamin D – RCT March 2018
Vitamin D supplementation for the treatment of non-alcoholic fatty liver disease: A randomized double blind placebo controlled trial.
Diabetes Metab Syndr. 2018 Mar 16. pii: S1871-4021(18)30006-7. doi: 10.1016/j.dsx.2018.03.006.
Dabbaghmanesh MH1, Danafar F2, Eshraghian A3, Omrani GR2.
BACKGROUND:
Low serum vitamin D has been associated with metabolic syndrome and Non-alcoholic fatty liver disease (NAFLD). This study aimed to investigate the impact of vitamin D supplementation in treatment of patients with NAFLD.
METHODS:
In a double blind, randomized, placebo controlled trial patients with NAFLD were randomized to receive one weekly pearl of placebo, 50,000 U vitamin D3 (cholecalciferol) pearl per week and 0.25 mg calcitriol (1,25 dihydroxycholecalciferol) pearl per day for 3 months.
RESULTS:
106 NAFLD patients were randomized to receive calcitriol, vitamin D3 and placebo pearls for 12 weeks and data for 91 patients were analyzed. After 12 weeks of treatment, serum alkaline phosphatase levels was significantly decreased from baseline levels in vitamin D and calcitriol treated groups (P < 0.05). Serum and gamma glutamyl transferase (GGT) level was also significantly decreased compared to the baseline levels after 12 weeks of treatment with vitamin D. There was no statistically significant difference between placebo, calcitriol, vitamin D groups in terms of serum aminotransferase, alkaline phosphatase, serum GGT and lipid profile (P > 0.05).
CONCLUSION:
While significant reduction of serum alkaline phosphatase and GGT were seen with vitamin D and calcitriol supplementation from baseline levels, no beneficial effects was seen when comparing vitamin D, calcitriol and placebo groups at the end of trial.
NAFLD not associated with Vitamin D genes – Mendelian analysis Feb 2018
Vitamin D and Nonalcoholic Fatty Liver Disease: Bi-directional Mendelian Randomization Analysis.
EBioMedicine. 2018 Feb;28:187-193. doi: 10.1016/j.ebiom.2017.12.027. Epub 2018 Jan 9.
Wang N1, Chen C1, Zhao L1, Chen Y1, Han B1, Xia F1, Cheng J1, Li Q1, Lu Y2.
BACKGROUND:
Vitamin D deficiency is associated with nonalcoholic fatty liver disease (NAFLD) in many cross-sectional studies. However, the causality between them has not been established. We used bi-directional mendelian randomization (MR) analysis to explore the causal relationship between 25-hydroxyvitamin D [25(OH)D] and NAFLD.
METHODS:
9182 participants were included from a survey in East China from 2014 to 2016. We calculated weighted genetic risk scores (GRS) for 25(OH)D concentration and NAFLD based on 25(OH)D-related and NAFLD-related single nucleotide polymorphisms. Presence of liver steatosis was assessed using ultrasound. Instrumental variable was used to measure the causal relationship between them.
RESULTS:
An SD increase in the 25(OH)D GRS was significantly associated with 25(OH)D (β 1.29, 95%CI -1.54, -1.04, P<0.05) but not with NAFLD (OR 0.97, 95%CI 0.92, 1.01). An SD increase in NAFLD GRS was also strongly associated with NAFLD (OR 1.09, 95%CI 1.04, 1.15, P<0.05) but not with 25(OH)D (β -0.15, 95%CI -0.41, 0.10). Using an instrumental variable estimator, no associations were found for genetically instrumented 25(OH)D with NAFLD and for genetically instrumented NAFLD with 25(OH)D.
CONCLUSION:
Our results support the conclusion that there is no causal association between vitamin D and NAFLD using a bi-directional MR approach in a Chinese population.
PMID: 29339098 PMCID: PMC5835542 DOI: 10.1016/j.ebiom.2017.12.027
📄 Download the PDF from VitaminDWiki
NASH – low response to 2,000 IU Vitamin D (15% vs 75%) – Oct 2017
Patients with Nonalcoholic Fatty Liver Disease Have a Low Response Rate to Vitamin D Supplementation.
J Nutr. 2017 Oct;147(10):1938-1946. doi: 10.3945/jn.117.254292. Epub 2017 Aug 16.
Dasarathy J1, Varghese R2, Feldman A2, Khiyami A3, McCullough AJ4, Dasarathy S4.
Background: Hypovitaminosis D is associated with an increased severity of nonalcoholic fatty liver disease (NAFLD), but reports on the response to cholecalciferol (vitamin D3) supplementation are conflicting.
Objective: The objective of this study was to determine if standard vitamin D3 supplementation is effective in NAFLD with hypovitaminosis D.Methods: Sixty-five well-characterized adults [age (mean ± SD): 51.6 ± 12.3 y] with biopsy-proven NAFLD were screened. Forty-two patients (the ratio of men to women was 13:29) had hypovitaminosis D (plasma 25-hydroxyvitamin D [25(OH)D] <30 ng/mL).
An observational study was performed in NAFLD patients with hypovitaminosis D treated with 2000 IU cholecalciferol (vitamin D3) daily for 6 mo per clinical practice. Plasma 25(OH)D, hepatic and metabolic panels, and metabolic syndrome components were assessed before and after cholecalciferol supplementation. Body composition was measured by using bioelectrical impedance analysis. The primary outcome measure was plasma 25(OH)D ≥30 ng/mL at the end of the study. Secondary outcomes included change in serum transaminases, fasting plasma glucose, and insulin and homeostasis model assessment of insulin resistance (HOMA-IR). Chi-square, Student's t tests, correlation coefficient, and multivariate analysis were performed.
Results: Twenty-six (61.9%) patients had nonalcoholic steatohepatitis (NASH), and 16 (38.1%) had hepatic steatosis. After 6 mo of cholecalciferol supplementation, plasma 25(OH)D ≥30 ng/mL was observed in 16 subjects (38.1%; responders) whereas the remaining 26 patients (61.9%) were nonresponders with plasma 25(OH)D <30 ng/mL.
Significantly fewer (P < 0.01) patients with NASH were responders (4 of 26, 15.4% ) than those with hepatic steatosis (12 of 16, 75% ). Baseline fasting serum alanine aminotransferase, plasma glucose, and HOMA-IR were similar in the responders and nonresponders, but the NASH score on the liver biopsy was lower (16.5%) in the responders (P < 0.001). Nonresponders had a higher fat mass (10.5%) and lower fat-free mass (10.4%) than responders did. End-of-treatment alanine aminotransferase and HOMA-IR improved only in responders. The baseline HOMA-IR and histological NASH score were independent predictors of nonresponse to cholecalciferol supplementation.
Conclusions: Daily supplementation with 2000 IU cholecalciferol for 6 mo did not correct hypovitaminosis D in the majority of patients with NASH. Further studies are needed to determine if higher doses are effective. This trial was registered at clinicaltrials.gov as 13-00153.
PMID: 28814531 PMCID: PMC5610550 [Available on 2018-10-01] DOI: 10.3945/jn.117.254292
Nearly 1 in 3 Americans have Nonalcoholic Fatty Liver Disease, and there are no symptoms - Nov 2019
NaturalHealth365
Recent Journal Articles
"Fatty liver disease linked with Metabolic Syndrome"
"A fatty liver often goes hand-in-hand with Heart Disease"
"Fatty liver disease is a risk factor for Dementia"
"A fatty liver imposes 91% higher risk for Cancer"
"Fatty liver disease is associated with a higher risk of stroke"
| GETTING OFF THE LIVER TRANSPLANT LIST | Burt Berkson, MD, PhD |
| TURNING AROUND AUTOIMMUNE HEPATITIS | Jessica Miner |
| STOPPING CIRRHOSIS + LIVER FAILURE | Denise Otten, H.H.C. |
| LIVER STRESS SIGNALS + GALLBLADDER ALERT | Dr. Robert DeMaria |
| RESTORING LIVER HEALTH NATURALLY | Dr. Peter Osborne |
| BALANCING THE LIVER PROPERLY | Thomas Lewis, PhD |
| THE BIG LIVER HEALTH-DISEASE PICTURE | Carlos Garcia, MD |