Down's syndrome and low vitamin D - several studies
Down's Syndrome and Vitamin D: Claude AI and Perplexity AI Aug 2025
Autoimmunity and Vitamin D deficiency in children affected with Trisomy 21 - 2018
Curr Pediatr Res 2018; 22 (3): 182-184
Moaz Othman Bokhari, Mohammed Fawzi Mujallid, Sultan Azizullah Alsulami, Asmaa Adel Milyani, Mohammed Abdulwakil Alsulami, Nader Nabil Malatani, Rayan Abdulrahim Al-Sharief, Mutlaq Ateeq Alsolami, Abdulmoein Eid Al-Agha aagha@kau.edu.sa
Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, Saudi Arabia.
📄 Download the PDF from VitaminDWiki
Background: Individuals with neurodevelopmental disorders and intellectual disabilities such as Trisomy 21 are more likely to experience low vitamin D levels, which has recently been tied to an increased risk of autoimmunity. In addition, Trisomy 21 is associated particularly with an increased incidence in coeliac disease and thyroid dysfunction. The aim of this study was to investigate the prevalence of autoimmune diseases and vitamin D deficiency in children affected with Trisomy 21.
Methodology: This is a retrospective study carried over the period of 12 years and included all children up to the age of 18 years. Data collected included laboratory reports such as profiles of both bone and thyroid, glycosylated haemoglobin A1C, fasting and random serum glucose levels; demographics such as age, gender and nationality; and diagnostic studies such as a tissue Transglutaminase (tTG) test and a duodenal biopsy. Data analysis was using the Statistical Package for Social Sciences v23.
Results: The prevalence of vitamin D deficiency was found to be 65.5% while the prevalence of coeliac disease and type 1 Diabetes Mellitus was found to be respectively 36.8% and 2.1%. Furthermore, 51.1% were found to be hypothyroid and another 22.6% to be hyperthyroid, leaving only 26.3% with a normal thyroid function.
Conclusion: We report a high incidence of vitamin D deficiency and autoimmune disorders, coeliac disease and thyroid dysfunction in particular, in children affected with Trisomy 21.
Introduction
The prevalence of Trisomy 21 (T-21) has been on the rise as a result of an increasing trend in maternal age coupled with a prolonged life expectancy of affected newborns [1,2]. In addition, the prevalence of autoimmunity in patients particularly affected with T-21 is augmented when compared to the general population [3]. Furthermore, evidence has brought into perspective that vitamin D receptors are now found on several immune cells and that vitamin D metabolites play a role in modulating the function of dendritic cells and the proliferation of T cells, concluding that vitamin D deficiency plays a role in development of autoimmune disorders [4,5]. Individuals with neurodevelopmental disorders and intellectual developmental disabilities, grouped into medically complex developmental disabilities (MCDD), were found to be particularly prone to having low serum concentrations of 1-25-hydroxycholecalciferol, shortly known as Vitamin D [6]. And according to the American Academy of Developmental
Medicine and Dentistry, T-21 was classified to be amongst the top most commonly diagnosed neurodevelopmental disorders [7]. Adequate vitamin D levels is found to be protective and is especially encouraged in children born with T-21 due to the aforementioned increased susceptibility to autoimmune dysfunction, encompassing thyroid dysfunction, coeliac disease, and type 1 Diabetes Mellitus, all of which already known to be in association with T-21 [8]. The aim of this study was to investigate the prevalence of Vitamin D deficiency, autoimmune thyroid dysfunction, coeliac disease and type 1 Diabetes Mellitus in the T-21 population.
Methodology
This study is a retrospective study that was carried out through reviewing electronic medical files using the Phoenix online medical records system implemented in KAUH to obtain necessary data. Files of patients from January 2005 till February 2018 were included. The sample size constituted 429 subjects. Inclusion criteria included patients affected with Trisomy 21 and exclusion criteria ruled out all those above 18 years of age.
Data collected included laboratory reports of bone profile, thyroid and metabolic profiles, thyroglobulin, and thyroid peroxidase, glycosylated haemoglobin A1C, fasting and random serum glucose levels; demographics such as age, gender and nationality; and diagnostic studies such as a tissue Transglutaminase (tTG) test and a duodenal biopsy.
Patients were considered vitamin D deficient/insufficient if levels of 25-Hydroxycholecalciferol were below 20 ng/ml, and normal if more than 20 ng/ml. They were also categorised into four groups based on their thyroid profile: Normal (TSH between 0.27-4.2 UIU/l and FT4 between 12.0-22.0 Pmol/l), Hypothyroid (if TSH>4.2 UIU/l and FT4<12 Pmol/l), Hyperthyroid (if TSH<0.27 UIU/l and FT4>22 Pmol/l), and subclinical hypothyroidism (TSH>4.2 UIU/l and FT4 between 12.0-22.0 Pmol/l). Furthermore, it was considered to be congenital if diagnosed up to 12 months of age in the setting of negative thyroid autoantibodies, whereas those who were older were considered to have an acquired form. Autoimmune thyroiditis was diagnosed in the setting of positive thyroid autoantibodies, thyroid peroxidase and anti-thyroglobulin.
With regards to coeliac disease, patients were considered latent if they had a high tTG in the setting of a normal biopsy and were positively diagnosed if they had a high tTG in the setting of positive biopsy. Fasting glucose 126 mg/dl random 200 mg/dl, HbA1C 6.5.
Informed consent was attained from the ethical committee at King AbdulAziz University Hospital prior to accessing patient files.
Data analysis
Data was interpreted using the 23rd version of the Statistical Package for Social Sciences (SPSS). Categorical data is presented in the form of numbers and percentages and continuous data in the form of mean ± standard deviation. Chi square test is used to compare the percentages between the groups and a p-value of <0.05 was chosen to represent statistical significance.
Results
Regarding demographics, 47.8% of the children were of the female gender. Means included current age and age at diagnosis, which were 6.55 years (SD ± 4.41) and 1.7 years (SD ± 2.9), respectively. The prevalence of vitamin D deficiency was found to be 65.5% while the prevalence of coeliac disease and type 1 Diabetes Mellitus were found to be respectively 36.8% and 2.1%. On the other hand, a thyroid profile was available for only 350 patients of our total sample size, of which 51.1% were found to be hypothyroid and another 22.6% to be hyperthyroid, leaving only 26.3% with a normal thyroid function. Regarding age at diagnosis, 72.3% cases of thyroid dysfunction belonged to the congenital category. Significance of gender played no role in autoimmunity for either disorder, with a respective p value of 0.92 and 0.89 for both coeliac and thyroid dysfunction.
Discussion
Trisomy 21 is considered to be yet the most common genetic cause of mental subnormality with an incidence of 1 in every 700-1000 live births [9]. Alongside general determinants of low vitamin D levels such as dietary factors and vitamin D supplements, which vary upon individual basis, is the high incidence of hypotonia amongst children affected with T-21. This is achieved by limiting their activity and exercise, which in turn leads to a shorter duration of outdoor time and consequent sun exposure [10]. Mental submentality is a known consequence of early onset thyroid dysfunction if not diagnosed and treated promptly, and therefore timely recognition and especially in the T-21 population cannot be stressed upon enough in order to prevent further deterioration in this already mentally impaired group. The lifetime prevalence of autoimmune thyroid dysfunction alone has reached up to 63% in the T-21 population, with up to 28 times the risk of development during the neonatal period, and a prevalence of up to 85% during infancy [11]. Similarly, our study showed that 72.3% of those who suffered thyroid dysfunction were diagnosed in the infancy period, with a total incidence of congenital hypothyroidism at 37%. This is matched by another study that concluded a 39% incidence of hypothyroidism within the first year of life [3]. However, in contrast, no cases of hyperthyroidism were found, while in our study, 22.6% of the patients were diagnosed with hyperthyroidism. Even then, we still conclude that hypothyroidism is more common in T-21 patients than hyperthyroidism as the prevalence was 51.1% of our total sample size. On the other hand, another study showed that all of the cases of hypothyroidism were acquired, occurring beyond the first year of life [12]. Although the majority of thyroid dysfunction encountered by our cases was of the congenital form, approximately 28% of them suffered the acquired form associated with autoimmunity. And while the female gender has been considered as an independent risk factor to the development of thyroid dysfunction, the role of gender in the onset of thyroid disease in the T-21 population was found to be not significant (p=0.89).
Children affected with T-21 are vulnerable to the delayed diagnosis of coeliac disease due to classical symptoms such as abdominal distention and discomfort, alteration in bowel habit, anaemia, and growth failure being attributed to the baseline disorder [13]. The prevalence of coeliac disease found by European studies amounted up to 17% in the T-21 population [14], while in American studies, was found up to 96 times more the risk encountered by the general population [15]. One study had shown that the prevalence of coeliac disease in the T-21 population was 5%, which reflected the general prevalence presumed by the United States [16]. Further European studies have shown a considerably higher increase in prevalence ranging from 7% up to 16% [14]. However, in either case, this is strongly contrasted by the prevalence estimated by our study, which approximated 37%. With regards to autoimmune insulin dependent Diabetes Mellitus, the prevalence in the T-21 population is thought to be around 1% [17]. The results shown by our study was not too far ahead as the prevalence was estimated to be at 2.1%.
Conclusion
In conclusion, we report a high incidence of both vitamin D deficiency and autoimmune disorders in children born with Trisomy 21 and recommend the screening and early diagnosis of both coeliac and thyroid disease in order to minimise the potential growth failure and mental submentality already anticipated with the syndrome alone. With regards to Diabetes Mellitus, while it is not as common as thyroid and coeliac disease, it is still a possibility and is seen in the T-21 population.
Consent for Publication: Consent was obtained from the patients’ legal guardian for this publication.
References (these start at #1,
Bittles AH, Bower C, Hussain R, et al. The four ages of Down syndrome. Eur J Public Health 2007; 17: 221-225.
Englund A, Jonsson B, Zander CS, et al. Changes in mortality and causes of death in the Swedish Down syndrome population. Am J Med Genet Part A 2013; 161: 642-649.
Pascanu I, Banescu C, Benedek T, et al. Thyroid dysfunction in children with Down’s syndrome. Acta Endocrinol (Copenh) 2009; 5: 85-92.
Christakos SDH. Vitamin D: Is there a role in extraskeletal health? Endocrinology 2011; 152: 2930-2936.
Reynolds GP, Warner CEJ. Amino acid neurotransmitter deficits in adult Down’s syndrome brain tissue. Neurosci Lett 1988; 94: 224-227.
Kilpinen-Loisa P, Arvio M, Ilvesmaki V, et al. Vitamin D status and optimal supplementation in institutionalized adults with intellectual disability. J Intellect Disabil Res 2009; 53: 1014-1023.
Grant WB, Wimalawansa SJ, Holick MF, et al. Emphasizing the health benefits of vitamin D for those with neurodevelopmental disorders and intellectual disabilities. Nutrients 2015; 7: 1538-1564.
Karlsson B, Gustafsson J, Hedov G, et al. Thyroid dysfunction in Down’s syndrome: Relation to age and Thyroid autoimmunity. Arch Dis Child 1998; 79: 242-245.
Weijerman ME, van Furth AM, Vonk Noordegraaf A, et al. Prevalence, neonatal characteristics and first-year mortality of down syndrome: A National Study. J Pediatr 2008; 152: 15-19.
Stagi S, Lapi E, Romano S, et al. Determinants of vitamin d levels in children and adolescents with Down syndrome. Int J Endocrinol 2015; 896758.
Carolina N, Mackey J. Hypo Thyroid ism in down syndrome: Screening guidelines and testing methodology. Am J Med Genet A 2004; 124A: 436-437.
Karlsson B, Gustafsson J, Hedov G, et al. Thyroid dysfunction in Down’s syndrome: Relation to age and Thyroid autoimmunity. Arch Dis Child 1998; 79: 242-245.
George EK, Mearin ML, Bouquet J, et al. High frequency of celiac disease in Down syndrome. J Pediatr 1996; 128: 555-557.
Zachor DA, Mroczek-Musulman E, Brown P. Prevalence of celiac disease in Down syndrome in the United States. J Pediatr Gastroenterol Nutr 2000; 31: 275-279.
Mackey J, Treem WR, Worley G, et al. Frequency of celiac disease in individuals with Down syndrome in the United States. Clin Pediatr (Phila) 2001; 40: 249-252.
Pueschel SM, Romano C, Failla P, et al. A prevalence study of celiac disease in persons with Down syndrome residing in the United States of America. Acta Paediatr Int J Paediatr 1999; 88: 953-956.
Pellegrini FP, Marinoni M, Frangione V, et al. Down syndrome, autoimmunity and T regulatory cells. Clin Exp Immunol 2012; 169: 238-243.
VitamiDWiki - Down syndrome people have even lower D levels if have additional Vitamin D diseases – Oct 2023
Vitamin D Deficiency in Preschool Children with Down Syndrome
Year 2021, Volume: 16 Issue: 3, 397 - 400, 01.11.2021 https://doi.org/10.17517/ksutfd.798173
Raikan BÜYÜKAVCI Mehmet Akif BÜYÜKAVCI
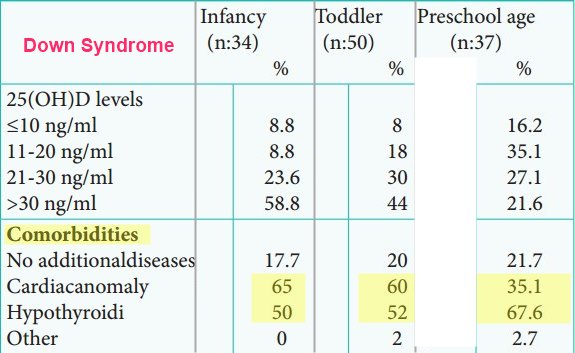
Vitamin D is a fat-soluble secosteroid prohormone that is produced on the skin by contact with sunlight. Through various metabolic changes in the body, it transforms into a hormone known as calcitriol, with a key role in the calcium and phosphate metabolism (1). Vitamin D serves plenty of functions in the body. Therefore, its deficiency may cause musculoskeletal symptoms such as bone pain, muscle weakness, gait difficulty, skeletal deformity, in addition to extraskeletal symptoms such as autoimmune diseases, cardiovascular diseases, and neuropsychiatric diseases (2).
Down Syndrome occurs as a result of trisomy, which occurs due to an extra copy of the whole or part of the long arm of chromosome 21 and is the most commonly known cause of delay in development. DS affects 1 in every 787 liveborn babies (3). DS is often accompanied by distinctive craniofacial features, congenital heart disease and immune, musculoskeletal and endocrine system abnormalities (4,5).
In patients with this syndrome, various environmental and hormonal factors such as hypotonia, low physical activity, poor calcium and vitamin D intake, intrauterine growth restriction, hypogonadism and thyroid dysfunction may contribute to bone mass and quality (6,7). Among all the others, vitamin D may have a crucial role in the health of these people. Vitamin D levels differ with many factors, including exposure to sunlight, dietary intake, and supplement use (8,9).
There is a lack of scientific evidence on the prevalence and severity of vitamin D deficiency in children with DS. Hence, this study aimed to determine vitamin D deficiency in children with DS, from infancy to toddler and particularly during the preschool period, and to raise awareness on the matter.
Download the PDF from VitaminDWiki
Down Syndrome low levels of Ca, Se, Zn – 2017
Systematic review and meta-analysis shows a specific micronutrient profile in people with Down Syndrome: Lower blood calcium, selenium and zinc, higher red blood cell copper and zinc, and higher salivary calcium and sodium
PLoS One. 2017; 12(4): e0175437. online 2017 Apr 19. doi: 10.1371/journal.pone.0175437
Amene Saghazadeh,1,2 Maryam Mahmoudi,3,4 Atefeh Dehghani Ashkezari,1,5 Nooshin Oliaie Rezaie,1,6 and Nima Rezaei1,6,7,*
Different metabolic profiles as well as comorbidities are common in people with Down Syndrome (DS). Therefore it is relevant to know whether micronutrient levels in people with DS are also different. This systematic review was designed to review the literature on micronutrient levels in people with DS compared to age and sex-matched controls without DS. We identified sixty nine studies from January 1967 to April 2016 through main electronic medical databases PubMed, Scopus, and Web of knowledge. We carried out meta-analysis of the data on
four essential trace elements (Cu, Fe, Se, and Zn),
six minerals (Ca, Cl, K, Mg, Na, and P), and
five vitamins (vitamin A, B9, B12, D, and E).
People with DS showed lower blood levels of
Ca (standard mean difference (SMD) = −0.63; 95% confidence interval (CI): −1.16 to −0.09),
Se (SMD = -0.99; 95% CI: -1.55 to -0.43), and
Zn (SMD = -1.30; 95% CI: -1.75 to -0.84),
while red cell levels of
Zn (SMD = 1.88; 95% CI: 0.48 to 3.28) and
Cu (SMD = 2.77; 95% CI: 1.96 to 3.57) were higher.
They had also higher salivary levels of
Ca (SMD = 0.85; 95% CI: 0.38 to 1.33) and
Na (SMD = 1.04; 95% CI: 0.39 to 1.69).
Our findings that micronutrient levels are different in people with DS raise the question whether these differences are related to the different metabolic profiles, the common comorbidities or merely reflect DS.
📄 Download the PDF from VitaminDWiki
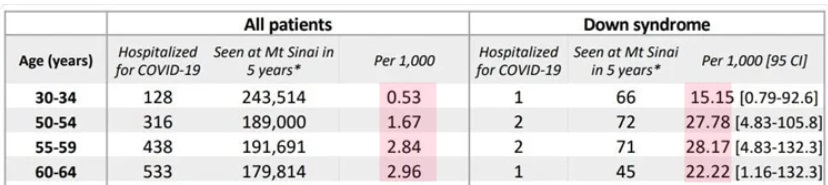
Down Syndrome associated with very low vitamin D - Oct 2023
Hypovitaminosis D in persons with Down syndrome and autism spectrum disorder
J Neurodev Disord . 2023 Oct 25;15(1):35. doi: 10.1186/s11689-023-09503-y.
Natalie K Boyd 1, Julia Nguyen 2, Mellad M Khoshnood 1, Timothy Jiang 1, Lina Nguyen 1, Lorena Mendez 1, Noemi A Spinazzi 3, Melanie A Manning 4, Michael S Rafii 5 6, Jonathan D Santoro 7 8
Background: Plasma levels of vitamin D have been reported to be low in persons with Down syndrome (DS) and existing data is limited to small and homogenous cohorts. This is of particular importance in persons with DS given the high rates of autoimmune disease in this population and the known relationship between vitamin D and immune function. This study sought to investigate vitamin D status in a multi-center cohort of individuals with DS and compare them to individuals with autism spectrum disorder (ASD) and neurotypical (NT) controls.
Methods: A retrospective, multi-center review was performed. The three sites were located at latitudes of 42.361145, 37.44466, and 34.05349. Patients were identified by the International Classification of Diseases (ICD)-9 or ICD-10 codes for DS, ASD, or well-child check visits for NT individuals. The first vitamin D 25-OH level recorded in the electronic medical record (EMR) was used in this study as it was felt to be the most reflective of a natural and non-supplemented state. Vitamin D 25-OH levels below 30 ng/mL were considered deficient.
Results: In total, 1624 individuals with DS, 5208 with ASD, and 30,775 NT controls were identified. Individuals with DS had the lowest mean level of vitamin D 25-OH at 20.67 ng/mL , compared to those with ASD (23.48 ng/mL) and NT controls ( 29.20 ng/mL ) (p < 0.001, 95% CI: -8.97 to -6.44). A total of 399 (24.6%) individuals with DS were considered vitamin D deficient compared to 1472 (28.3%) with ASD and 12,397 (40.3%) NT controls (p < 0.001, 95% CI: -5.43 to -2.36). Individuals with DS with higher body mass index (BMI) were found to be more likely to have lower levels of vitamin D (p < 0.001, 95% CI: -0.3849 to -0.1509).
Additionally, having both DS and a neurologic diagnosis increased the likelihood of having lower vitamin D levels (p < 0.001, 95% CI: -5.02 to -1.28). Individuals with DS and autoimmune disease were much more likely to have lower vitamin D levels (p < 0.001, 95% CI: -6.22 to -1.55). Similarly, a history of autoimmunity in a first-degree relative also increased the likelihood of having lower levels of vitamin D in persons with DS (p = 0.01, 95% CI: -2.45 to -0.63).
Conclusions: Individuals with DS were noted to have hypovitaminosis D in comparison to individuals with ASD and NT controls. Associations between vitamin D deficiency and high BMI, personal autoimmunity, and familial autoimmunity were present in individuals with DS.
📄 Download the PDF from VitaminDWiki
Endocrinal dysfunction in children with Down syndrome - 2022
Many endocrine problems that might be helped by Vitamin D supplementation
📄 Download the PDF from VitaminDWiki
Down Syndrome review (Vitamin D not mentioned) 2022
📄 Download the PDF from VitaminDWiki