Obese teens need more than 2,000 IU of vitamin D for 3 months– RCT
Cholecalciferol supplementation does not influence β-cell function and insulin action in obese adolescents: a prospective double-blind randomized trial.
J Nutr. 2015 Feb;145(2):284-90. doi: 10.3945/jn.114.202010. Epub 2014 Dec 17.
Javed A1, Vella A2, Balagopal PB3, Fischer PR4, Weaver AL5, Piccinini F6, Dalla Man C7, Cobelli C7, Giesler PD8, Laugen JM8, Kumar S9.
1Divisions of Pediatric Endocrinology and.
2Division of Endocrinology and Metabolism.
3Nemours Children's Clinic, Research Division, Jacksonville, FL; and.
4General Pediatric and Adolescent Medicine, Department of Pediatric and Adolescent Medicine.
5Division of Biomedical Statistics and Informatics, Department of Health Sciences Research, Mayo Clinic, Rochester, MN.
6Information Engineering and.
7Department of Electronics and Informatics, University of Padua, Padua, Italy.
8Endocrine Research Unit, Division of Endocrinology, Diabetes, Metabolism, and Nutrition, Department of Internal Medicine, and.
9Divisions of Pediatric Endocrinology and kumar.seema@mayo.edu.
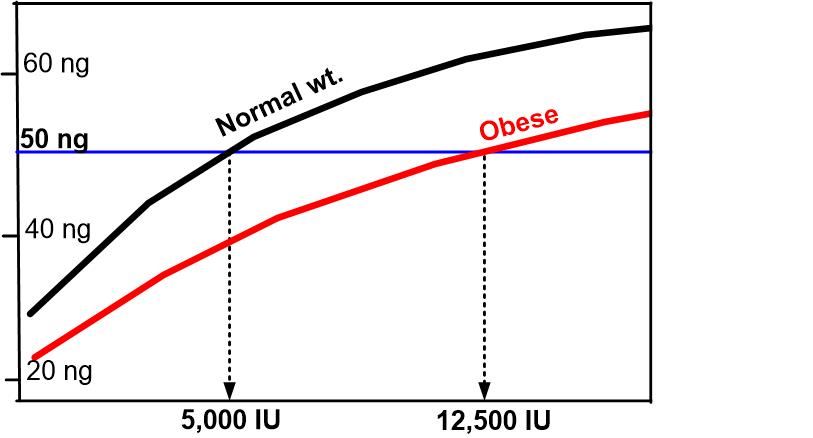 * __Normal weight Obese (50 ng = 125 nanomole)__
click Here for details
* __Normal weight Obese (50 ng = 125 nanomole)__
click Here for details
BACKGROUND: There is increasing interest in the extraskeletal effects of vitamin D, particularly in the obese state with regard to the development of insulin resistance and diabetes.
OBJECTIVE: The objective of the study was to determine the effect of 2 doses of cholecalciferol (vitamin D3) supplementation on insulin action (Si) and pancreatic β-cell function in obese adolescents.
METHODS: We performed a 12-wk double-blind, randomized comparison of the effect of vitamin D3 supplementation on Si and β-cell function in obese Caucasian adolescents (body mass index > 95(th) percentile). The subjects were randomly assigned to receive either 400 IU/d (n = 25) or 2000 IU/d (n = 26) of vitamin D3. Each subject underwent a 7-sample 75 g oral glucose tolerance test, with glucose, insulin, and C-peptide measurements, to calculate Si and β-cell function as assessed by the disposition index (DI), with use of the oral minimal model before and after supplementation. A total of 51 subjects aged 15.0 ± 1.9 y were enrolled. Included for analysis at follow-up were a total of 46 subjects (20 male and 26 female adolescents), 23 in each group.
RESULTS: Initial serum 25-hydroxyvitamin D [25(OH)D] was 24.0 ± 8.1 μg/L. There was no correlation between 25(OH)D concentrations and Si or DI. There was a modest but significant increase in 25(OH)D concentration in the 2000 IU/d group (3.1 ± 6.5 μg/L, P = 0.04) but not in the 400 IU/d group (P = 0.39). There was no change in Si or DI following vitamin D3 supplementation in either of the treatment groups (all P > 0.10).
CONCLUSIONS: The current study shows no effect from vitamin D3 supplementation, irrespective of its dose, on β-cell function or insulin action in obese nondiabetic adolescents with relatively good vitamin D status. Whether obese adolescents with vitamin D deficiency and impaired glucose metabolism would respond differently to vitamin D3 supplementation remains unclear and warrants further studies. This trial was registered at clinicaltrials.gov as NCT00858247.
© 2015 American Society for Nutrition.
PMID: 25644349