Table of contents
- Natural Immunity Vs. Vaccination
- How I Selected the Data
- The Clinical Trials (Pre-Delta)
- Pre-Delta Observational Studies
- A Study Covering the Whole of Israel
- Since only one single person in the entire country died of a second infection,
the stats couldn't be done on natural immunity and death. - The Two Time-Matched Delta Studies
- Hybrid Immunity
- I can say nothing more except that hybrid immunity deserves much more study.
- Conclusions
- Video With Q and A
- Subscribe
- Please Support This Service
- Footnote *
- VitaminDWiki
Natural Immunity Vs. Vaccination
Original on the web
Disclaimer: I am not a medical doctor and this is not medical advice. My goal is to empower you with information. I will not take a position on whether you should or should not get vaccinated. Please make this decision yourself, consulting sources you trust, including a caring health care professional.
What provides better protection against COVID, natural immunity, or vaccination?
When asking this question, we should step back and ask why we are asking it.
I am not posing the question to ask whether we should go out and deliberately contract COVID. I believe, instead, we should protect ourselves from COVID.
The main reason we ask this question is because we want to know whether people who have already gotten COVID need to get vaccinated in order to obtain a similar level of immunity obtained by people who have gotten vaccinated but have never gotten infected. Stepping further back, there are two reasons we could be asking this:
- If I've had COVID, can I make myself more immune than I already am by getting vaccinated?
- If we assume that anyone who gets infected can spread COVID, do we need to force everyone who has had COVID already to get vaccinated so they can enter a public place, keep their job, or otherwise participate in society, to stop them from spreading it?
If we are asking this question for the first reason, then we want high-quality, well-controlled, cause-and-effect data. We want to have a strong idea of what the vaccine would do within us to boost our own immunity if we take it. We are after the biological fact of what it is doing.
If we are asking this question for the second reason, as in evaluating the rationale for vaccine mandates, we do not want highly controlled data. We want fully confounded data. We want to know if we take random people off the street, are those who have had COVID but haven't gotten vaccinated any more or less dangerous to be around than those who haven't had COVID but have gotten vaccinated? The bouncer at the restaurant isn't going to use some sophisticated statistical analysis and has no need to understand biology. The bouncer is trying to filter out the safe people from the dangerous people.
Let's try to tackle this from both perspectives.
How I Selected the Data
I searched pubmed, biorxiv, medrxiv, and SSRN for peer-reviewed papers and preprints* that compared the infection risk of unvaccinated people who have had COVID to vaccinated people who haven't had COVID. I excluded studies that looked just at antibodies, T cells, or other markers of immunity. Since none of these have been validated as predictors of infection risk across the populations we are concerned with (everyone who has or hasn't had COVID and everyone who has or hasn't been vaccinated), these can only help us explain what we observe in infection risk, or help us hypothesize something about infection risk. They don't actually tell us the infection risk. So I focused exlcusively on studies that tell us the difference in infection risk, and I found nine of them.
The Clinical Trials (Pre-Delta)
Although randomized controlled trials (RCTs) are the gold standard of cause-and-effect evidence, for our question even the RCTs are just observational studies. This is because the vaccine trials randomized vaccination, but didn't randomize previous COVID infection.
The two trials that reported infection risk for vaccination and previous infection separately were the Pfizer trial and the Astrazeneca trials. Both of them were done before the delta variant took hold, and both of them appear to have defined previous infection based simply on a baseline blood sample that tested positive for nucleocapsid antibodies. These are antibodies that you make to natural infection, but not to vaccination. In both cases, people only got PCR tests if they had COVID symptoms. So we can't separate out getting infected from becoming a symptomatic case.
In both cases, we have no idea how long before the trial the previous infections were. We just know that previously infected people were infected at some point during the pandemic. Many of the natural infections could have been 9-12 months old by the time people experienced subsequent infections. We also don't know how many of the natural infections were even strong enough for the people to notice they had them. We just know they tested positive for antibodies. In other words, these people may never have been sick.
In the Astrazeneca trials, where people were followed for an average of 3.4 months, the unvaccinated, never-infected placebo participants had a 1.7% risk of developing symptomatic COVID, while the risk was 0.8% in unvaccinated people with previous infection, and was 0.5% in those who were never infected but got vaccinated.
In the Pfizer trial, where a slight majority of people were followed for 4-6 months and most of the others were followed for less, the never-infected placebo participants had a 4.7% chance of becoming a symptomatic COVID case, the naturally infected had a 1.3% chance, and the never-infected vaccinated had a 0.5% chance. Those who had both natural infection and vaccination had a 0.4% chance.
These studies were not done to compare the relative effects of natural infection and vaccination. They were just done to test the effect of vaccination. Those who had evidence of previous infection were tracked primarily to exclude them from the main analysis. As such, they didn't perform stats on the protective effect of natural infection. The Pfizer trial did, however, do stats on the effect of vaccination within people who had evidence of natural infection, and it wasn't statistically significant.
Nevertheless, in these trials run by the vaccine manufacturers themselves, done prior to the delta variant taking hold, using nothing more than a blood test for antibodies as evidence of natural infection, where natural infections could have been 9-12 months old, natural immunity looks 53-72% effective at protecting against becoming a symptomatic COVID case, and being vaccinated on average 3-4 months ago looks 70-90% effective.
Pre-Delta Observational Studies
A number of observational studies were done prior to the delta variant taking hold:
- Among staff in publicly funded hospitals within the UK when the alpha variant was dominant, the rollout of the Pfizer vaccine was studied for two months. Everyone got PCR tests every two weeks and previous infection status was taken from medical records based on a previous PCR or antibody test. The age of the natural immunity was unknown or unreported, but the vaccinations were only up to two months old. For every 100,000 person-days, the chance of a positive test was 20 with no immunity, 5 with Pfizer, 3 with natural immunity, and 2 with hybrid immunity (Pfizer and natural). This suggests that a very recent Pfizer vaccine is 75% effective, an older case of natural immunity is 85% effective, and combining the two adds a little extra boost — at least over a two-month period.
- In long-term care facilities in the UK during the alpha variant, where everyone was over 65 and the median age was 86, the rollout of Pfizer and Astrazeneca was observed over 3 months. People got tested every month, and were also tested if they got sick or if there was an outbreak. A positive PCR or antibody test was used to define natural infections. The age of the natural infections were unknown or unreported, but the vaccinations were no more than 3 months old. The vaccines reduced the risk of testing positive by 64%, while natural immunity reduced the risk by 88%. Adding a vaccine to natural immunity had no benefit, not even a trend toward a benefit. In this population, older natural immunity was almost 40% more effective than more recent vaccination.
- In long-term care facilities within Spain, where everyone was over 65 and the mean age was 86, the rollout of Pfizer and Moderna (almost entirely, 99.8%, Pfizer) was studied over 2.5 months. Testing was done whenever anyone had symptoms, was considered at risk of exposure, or was new to the facility. In this study they wanted to separate the effect of natural immunity from the indirect effect of widespread vaccination, so they compared two different time periods: the protective effect of natural infection in mostly 2020 was compared to the protective effect of vaccination in 2021. The natural infections were on average 6 months old, while the vaccinations were only up to 2.5 months old. Per 100,000 person-days, the risk without immunity was 12.8, with vaccination was 5.4, and with natural immunity was 1.8. Combining vaccination and natural immunity brought this down to 1.13. While this shows a slight boost of the combination, the natural immunity alone is three times better than the vaccine.
- In a preprint* covering the four-month rollout of Pfizer and Astrazeneca among the staff of a cancer center in Milan, Italy, the protective effect of the vaccine over the rollout was compared to the protective effect of natural infection over a previous 8-month period. During both periods, PCR testing was done at the beginning and end of the period, upon development of symptoms or a positive antibody test, after holidays, and, for doctors, every two weeks. The natural infections were up to 8 months old while the vaccinations were on average two months old. The infection rate among those with no immunity was 9.5%, and among vaccinated was 1.5%. Natural immunity looked better or worse than vaccination depending on what method of PCR testing was used. If they tested a single gene, the reinfection rate was 3%. But if they tested multiple genes, which is more reliable, the reinfection rate was less than 1%. Overall this study is not very good for forming conclusions, but older natural infection looks comparable to more recent vaccination.
These studies have the advantage of being done in real-world scenarios outside the control of the vaccine manufacturers. They all suggest that an older case of natural immunity is equal to or substantially better than a more recent vaccination, and they conflict as to whether adding a vaccination will make natural immunity even better.
A Study Covering the Whole of Israel
By far the largest study is a preprint* covering the entire country of Israel from June 1, 2020 to March 20, 2021. This covers the period when the alpha variant was dominant, when Pfizer was the exclusive vaccine used. PCR testing was free and generally ordered because someone was sick or was exposed to someone who was sick. Previous infections were 2-10 months old, and vaccinations were 0-3 months old. The more recent vaccination was 93% effective against infection, 94% against hospitalization, 94% against severe illness, and 94% against death. Older cases of natural immunity were 95% effective against infection, 94% against hospitalization, and 96% against severe illness.
Since only one single person in the entire country died of a second infection,
the stats couldn't be done on natural immunity and death.
In by far the largest study, old natural immunity is shown to be equivalent to recent vaccination.
The Two Time-Matched Delta Studies
Two preprints* cover the time period when delta became dominant, which is important because delta may evade immunity from spike protein-based vaccines more effectively than natural immunity. These are also the only two studies in the entire batch that compare vaccinations and natural infections that happened at the same time. This is critical, because immunity of any type can wane over time, so we only appreciate the relative strength of each when they are equally fresh.
One was done in Israel, and the other in the United States. On the whole, the US study was designed to replicate the Israeli study by covering the same time period, focusing on the delta variant, and matching people according to their demographics, risk factors, and when they got infected or vaccinated. In both cases, previous infections were drawn from electronic medical records. In Israel, it was from the second-largest HMO. In the US, it was from the Veterans Health Administration. The main differences between the two studies is that the patients in the US study were older (on average 62 instead of 33-36), and that Israel used Pfizer whereas the US study used a combination of Pfizer and Moderna.
In the Israeli study, natural infection offered 13-fold better protection against infection, 27-fold better protection against developing symptoms, and 8-fold better protection against hospitalization.
When the Israeli study used a group that was twice as big but not matched for the time of vaccination or infection, natural immunity was 6-fold more protective against infection and 6.7-fold more protective against hospitalization. No one in the Israeli study died.
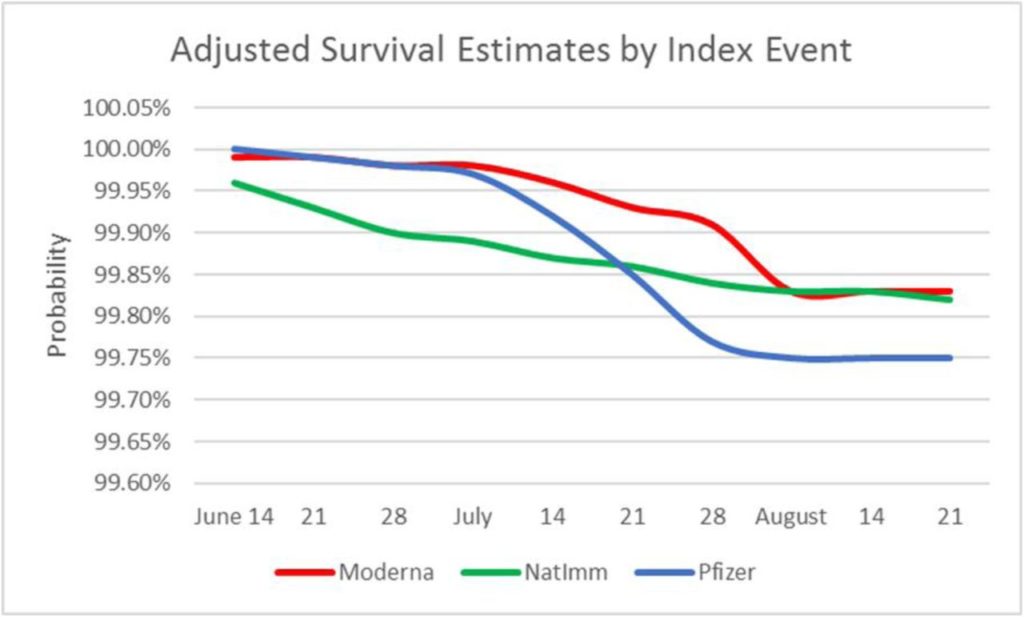
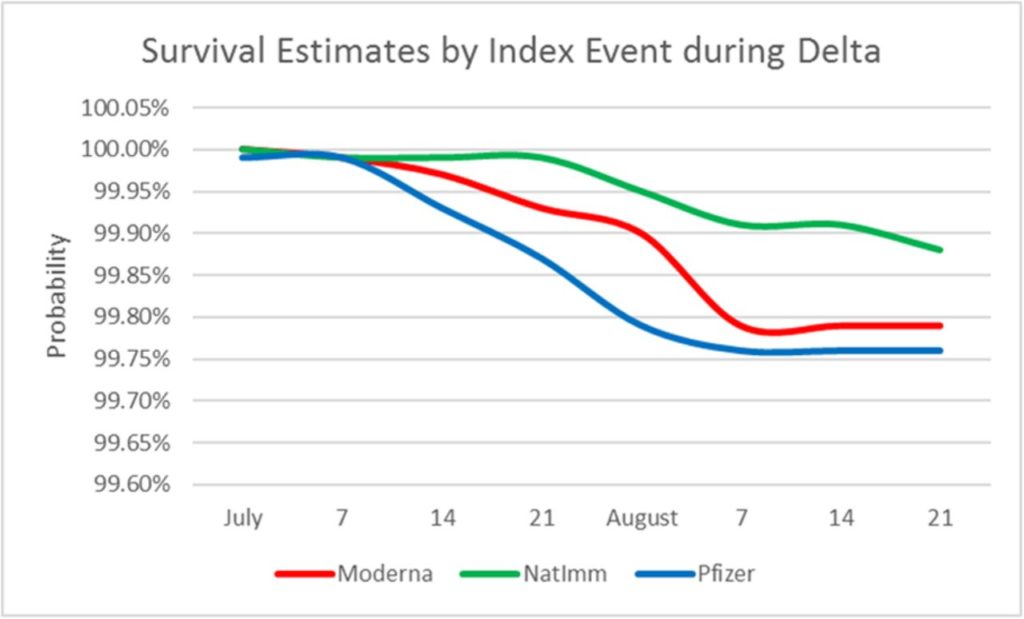
At first glance, the US study appears to suggest the vaccines work better than natural immunity for people over 65, but not for younger people. For seniors, they offered 66% lower risk of infection and hospitalization and 95% lower risk of death. However, the study covered June through August of 2021, and delta didn't reach close to 100% of infections until July and August. By August, natural immunity had become equivalent to Moderna and superior to Pfizer.
Their figures are not well explained, but they appear to represent, first, the data adjusted for time of natural infection or vaccination, demographics and risk factors, and then the unadjusted data. In the first figure, natural immunity (green) becomes equivalent to Moderna (red) and superior to Pfizer (blue) by August. In the second figure with the unadjusted data, natural immunity becomes superior to both by mid-July, and widens its superiority by August.
Hybrid Immunity
Studies conflict on whether vaccination and natural immunity combined offer some superior advantage. The Israeli delta study suggested that the combination might cut the risk of infection in half compared to having just natural immunity alone (as if 27-fold better protection against being a symptomatic case wasn't enough!)
When they looked at people vaccinated after previous infection, which is most relevant to the question of whether someone who has been infected already should get vaccinated, this additional benefit was not statistically significant, but it looked like a 40% lower risk.
Similarly, in the Pfizer trial, adding vaccination on top of natural infection looked like it provided a 60% further drop in infection risk, but wasn't statistically significant.
A CDC study (in MMWR, which is not peer-reviewed) done in Kentucky from May to June of this year found a statistically significant 43% lower risk of infection when vaccination was thrown on top of natural infection.
Conversely, a preprint* covering health care workers in India found that those with natural immunity prior to vaccination had an additional 74% reduction in risk of infection compared to those who were vaccinated and never infected.
Nevertheless, at least one study contradicts the hybrid immunity concept. As I noted above, in long-term care facilities in the UK there was no benefit of adding vaccination to natural infection. It's not just that it's not statistically significant. Supplementary table 5 shows that, with time from adding the vaccination, the relative risk compared to natural immunity alone swings up and down all over the place.
I also wonder about other types of hybrid immunity. For example, if we could know we have a certain amount of established immunity already, would relaxing our guard just a little get us more exposure to dead viral fragments on surfaces and to mini-boosts of exposure to the live virus that are below the minimum infectious dose? I realize that we need to learn a lot before we can define what is safe and what is dangerous here, but there seems to be a broad spectrum of hybrid immunity concepts that should be explored.
I also wonder whether vaccination after natural infection wouldn't narrow the immunity from a broader spectrum of targets more resilient to a rapidly changing variant landscape toward the original spike protein that is becoming less and less relevant to the COVID we face here and now as time goes on.
I can say nothing more except that hybrid immunity deserves much more study.
Conclusions
The only studies that make the vaccines look better than natural immunity are the vaccine trials, and a surface reading of the US delta study. Reading the US delta study carefully makes natural immunity begin to show its superiority as delta fully takes over. Every other study clearly shows that older natural immunity is equal to or superior to more recent vaccination. When natural infections and vaccinations occur at the same time in a fully delta-dominant environment, natural immunity appears to be superior. In the younger population of Israel it seems to be wildly superior to the Pfizer vaccine. In by far the largest study covering the entirety of Israel, old natural infection is every bit as good as recent vaccination against infection, symptomatic illness, and hospitalization.
The only reason we can't say that about death is because only one single person died of a second infection in the whole of Israel!
To answer the questions at the beginning:
Does someone with natural immunity need to get vaccinated to obtain equal immunity to the vaccinated around them?
- Definitely not. Their immunity at worst is just as good.
Will they get even better immunity if they add vaccination?
- They might, but the studies conflict.
Can I decide who to fire from their job, who to keep out of the gym, and who to keep out of the restaurant by considering people with natural immunity dangerous unless they've been vaccinated?
- Definitely not! If anything is obvious pseudoscience, it is this.
These data show that simply having an antibody test or a previous PCR test is enough to show that, even when your infection is way older than someone else's vaccination, it is equal to or better in its protection. Not allowing a mere anti-nucleocapsid antibody test or any record of any positive PCR test to serve as equal proof of immunity to a vaccination card is scientifically unjustifiable.
Video With Q and A
Subscribe
Click here to subscribe to my COVID-19 Research Updates newsletter.
Please Support This Service
You can support this service by sharing my work with others to spread the word, and by purchasing one of my information products. The most popular are:
The Vitamins and Minerals 101 Cliff Notes
Testing Nutritional Status: The Ultimate Cheat Sheet
Vitamins and Minerals 101: (pre-order the book and get the COVID guide for free)
There are many other ways to support this work, some at no extra cost to you, listed at chrismasterjohnphd.com/support.
Over the next several weeks, I'm going to be devoting my analytical skills to critical questions around COVID risks, vaccine safety and efficacy, and the full spectrum of vaccine alternatives, due to the imminent massive job loss occurring as a result of vaccine mandates. If you would like to support me doing this work you can also make a donation in any amount using this button:
chrismasterjohnphd.com/donate
Footnote *
* The term “preprint” is often used in these articles. Preprints are studies destined for peer-reviewed journals that have yet to be peer-reviewed. Because COVID-19 is such a rapidly evolving disease and peer-review takes so long, most of the information circulating about the disease comes from preprints.
VitaminDWiki
Natural immunity to SARS (at least 10 months SARS-2, 17 years SARS-1)
VitaminDWiki pages with VACCIN in the title (94 as of Oct 2021)
VACCINation, VACCINations, VACCINes, VACCINe, VACCINated, etc.
List is automatically updated
VitaminDWiki pages with Masterjohn in the title (16 as of Oct 2021)
List is automatically updated
COVID-19 treated by Vitamin D - studies, reports, videos
- As of March 31, 2024, the VitaminDWiki COVID page had: trial results, meta-analyses and reviews, Mortality studies see related: Governments, HealthProblems, Hospitals, Dark Skins, All 26 COVID risk factors are associated with low Vit D, Fight COVID-19 with 50K Vit D weekly Vaccines Take lots of Vitamin D at first signs of COVID 166 COVID Clinical Trials using Vitamin D (Aug 2023) Prevent a COVID death: 9 dollars of Vitamin D or 900,000 dollars of vaccine - Aug 2023
5 most-recently changed Virus entries