Vitamin D Obesity therapy should start with 50,000 IU weekly - Dec 2025
Is vitamin D deficiency a risk factor for obesity-related morbidity, prediabetes, and type 2 diabetes - a literature review and proposals from the experts of the Polish Society of Endocrinology
Endokrynol Pol . 2025;76(6):579-585. doi: 10.5603/ep.109313.
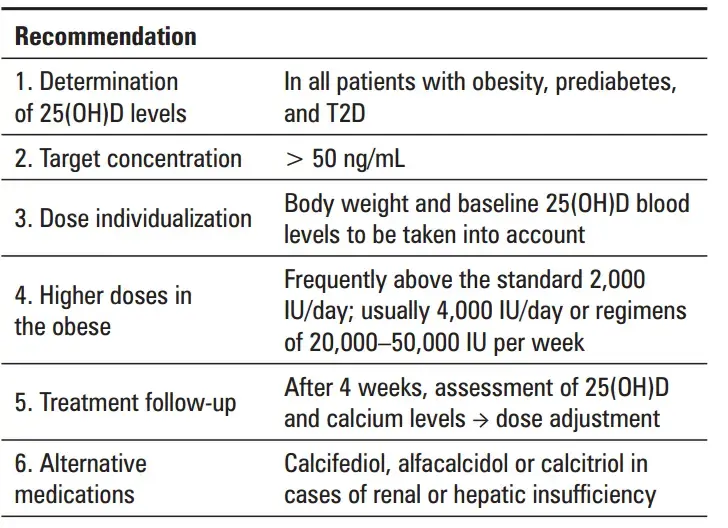
Through pleiotropic effects related to the presence of its receptors in major human organs, vitamin D (VD) plays an important role in systemic homeostasis, especially in the proper functioning of muscles and bones. In light of the published data from both animal and human studies, VD deficiency should be considered a risk factor for obesity-related morbidity, prediabetes, and type 2 diabetes (T2D); in addition, VD supplementation in VD deficiency has a beneficial effect on the effects of treatments aimed at normalization of body weight (including incretin drugs) and the metabolism of carbohydrates in prediabetes and T2D. The objective of this paper is to present the current knowledge and evidence on the relationship between VD deficiency and obesity, prediabetes, and T2D. The paper is intended to be used as a practical guide. The authors propose that serum 25(OH)D concentrations be determined in adults who are obese or overweight (i.e., belonging to the group presenting with a multiple increase in the risk of VD deficiency) or adults who are obese or overweight and have prediabetes or T2D. The baseline VD levels should determine the therapeutic dose and be helpful in assessing the effectiveness of therapy. The available literature lacks precise information regarding the recommended doses of VD in obese people, with 4000 IU being a frequently suggested daily dose. Most papers recommend that body weight be taken into account when determining the dose of VD in the obese; the dose should be higher than in individuals with normal body mass index (BMI). The authors suggest that in the case of low VD levels (< 20.0 ng/mL), quite frequently as low as 12.0-15.0 ng/mL, in an adult obese patient, VD therapy should be started at 20,000 IU two times per week or 50,000 IU once a week with 25(OH)D and calcium levels being checked after one month so that a decision can be made on the further course of therapy. The suggested 25(OH)D concentration target range is > 30-50 ng/mL. In a patient-tailored supplementation model, the dose of VD should depend on body weight and, most importantly, on the baseline VD level.
In the absence of the expected effects, the authors suggest that the dose of VD (usually vitamin D3) be increased or the treatment be switched to calcifediol or alfacalcidol, or calcitriol in special cases such as impaired kidney or liver function. It is important to emphasize the need to individualize the management and monitor blood calcium and creatinine levels during chronic VD therapy, including high-dose therapy.