Vitamin D interview and transcript - Dr. Boucher- Jan 2026
Summary of Vitamin D, Insulin Resistance, and Metabolic Disease by Google AI
Restoration of Insulin Secretion (07:51):
Dr. Boucher highlights early research indicating that Vitamin D replacement can boost insulin secretion back to normal levels in deficient individuals, identifying deficiency as a major aggravator of metabolic syndrome.
Local Activation in Metabolic Tissues (19:22):
Unlike bone health, which relies on kidney activation, metabolic target tissues (liver, muscle, and pancreatic islets) activate Vitamin D locally from circulating 25(OH)D. This process is independent of parathyroid hormone (PTH) and depends solely on the availability of the substrate in the blood.
The Obesity and Diabetes Impairment (20:31):
Both obesity and diabetes suppress the liver enzyme responsible for producing 25(OH)D. As a result, obese or diabetic individuals may require up to three times the standard dose of Vitamin D to achieve the same circulating blood levels as leaner individuals.
Ineffectiveness of Bolus Dosing (21:22):
Dr. Boucher explains that large, infrequent "bolus" doses often fail to heal conditions like rickets or improve metabolic health because they trigger the body's protective mechanisms to break down Vitamin D. Consistent daily dosing is proven to be significantly more effective.
Long-Term Trajectory of Insulin Resistance (23:25):
Data from long-term cohorts like the Whitehall study show that insulin resistance begins to rise 10 to 20 years before a clinical diagnosis of type 2 diabetes, emphasizing the need for early and sustained Vitamin D repletion throughout life.
Target Blood Levels for Disease Prevention (36:06):
A re-analysis of the D2D trial revealed that maintaining serum levels above 100–125 nmol/L (40–50 ng/mL) reduced the risk of type 2 diabetes by over 70%. Achieving these levels often requires daily supplementation of at least 4,000 IU.
Optimization via Fatty Meals (53:31): Because Vitamin D is fat-soluble, its absorption is significantly enhanced when taken with the day's largest or fattest meal rather than on an empty stomach.
The "Orchestra" of Co-nutrients (55:45):
Vitamin D does not work in isolation; it requires co-factors like Magnesium and Vitamin K2 for proper activation and endothelial protection. Recent insights suggest that high magnesium intake strengthens the association between Vitamin D and improved insulin sensitivity (Source).
Public Health and Negligence (40:44):
Dr. Boucher concludes that failing to correct widespread Vitamin D deficiency at a population level—especially given its low cost and high safety—is a form of public health negligence that contributes to the global "pandemic" of metabolic disease.
Related in VitaminDWiki
- Daily, weekly, and bi-weekly VitaminD dosing got to the same level
- Many symptoms vanquished by Vitamin D (50,000 IU weekly)
- Weekly, Monthly Vitamin D are typically better than daily - many studies
- Health can be greatly improved by weekly 50,000 IU of Vitamin D - video Lahore
- Weekly Vitamin D better than daily – lower cost, less pill burden, perhaps 1.5X better response – meta-analysis
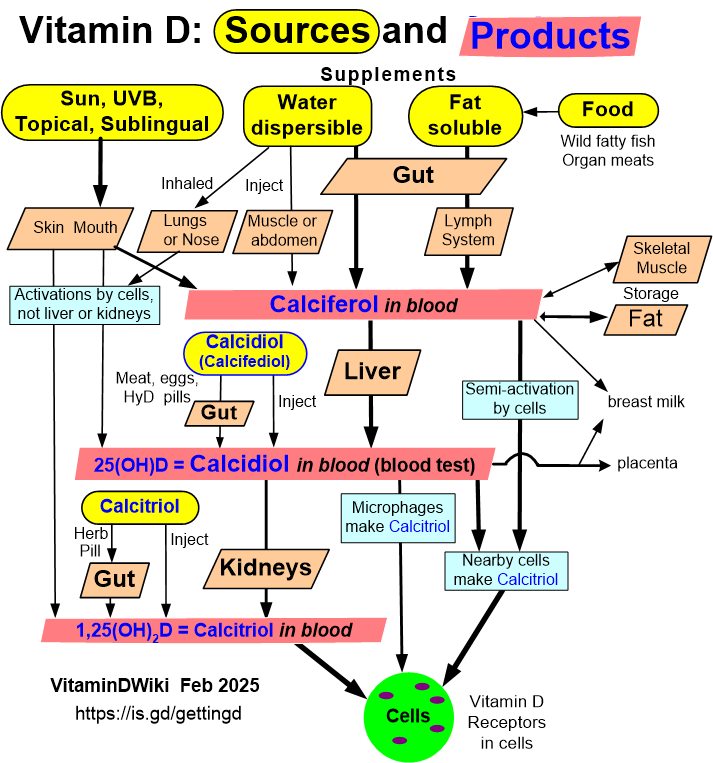
Dr. Boucher believes in the light blue pathways
Full transcript
Well, I'd like to officially welcome everybody to today's vitamin D study hour. And I am so happy to have Dr. Barbara Buchet here today uh to discuss the relationship between vitamin D and the risk of metabolic syndrome, insulin resistance, and type 2 diabetes. And uh two of the publications that we decided to feature for today's study hour um are uh co-authored or authored by Dr. Buché.
(00:41) And I do want to mention she's published so many other papers. She's been doing this for decades. Um and I did recently uh share another paper that she co-authored. I believe it was uh published last year. So if anybody wants copies of these papers, I sent links to these papers as well before the study hour, just let me know.
(01:05) So a little bit about Dr. Boucher. Uh she is retired, but she was honorary professor of metabolic medicine. Um she has more than 50 years of research and clinical experience. She has worked as a consulting physician in general and emergency medicine. uh she was a senior lecturer in diabetes and metabolic medicine and her research since has primarily focused on vitamin D deficiency and human disease including environmental risk factors such as beetle chewing and metabolic health.
(01:44) Um so and as I mentioned she has authored many papers over 160 peer-reviewed publications and uh she has collaborative collaborated extensively on large international cohort studies examining vitamin D metabolic syndrome diabetes and cardiovascular risk across the life course. So a few notes before I hand it over u please submit your questions for Dr.
(02:12) Buché at the end to the question and answer section and we will answer all questions that were submitted prior to the study study hour today and during the study hour uh after Dr. Buché's presentation. Um we will be recording this and it will be posted to our YouTube and website and I will also email the link to everybody.
(02:38) And of course, just a little bit about grassroots health and our vitamin D action study. You can join our de action study and measure your vitamin D levels at home along with other important markers and join join our cohort. And by doing that, you are supporting the all the work of grassroots health including these study hours.
(02:59) Um, and I'm going to say my thanks now. Again, email me jen@grassrooshealth.org with any questions, feedback, stories. Donations are always welcomed and appreciated and I want to thank those who support us and sponsor us. And with that, I am going to hand it over to Dr. Buché. >> Thank you very much. I'm very honored to be able to join you to talk about a topic that I've worried away at for as you've heard many decades.
(03:29) The talk presentation arose from a particular paper in 2020 which provides the title. you can see now. Um, I hope that what I'm going to tell you or show you will perhaps improve your confidence that getting your vitamin D supplementation adequate should reduce insulin resistance, which has a very good chance of reducing the risks of getting type 2 diabetes.
(03:58) Next slide, please. Next slide. Thank you. My background, how I got into all this really goes back as you heard a long way. Um the the National Health Service in Britain set up in 1948, one of its amuse amusements was that it forced all British medical schools to accept 12% of their students as women for the first time and I was one of them.
(04:27) Very shortly afterwards, I did an intercolated BC where I learned, you know, watched people doing research and got some idea of how how it worked and how one people thought about it. And um I also did a little project um while I was doing that BC sexing fetal bones from white fetuses because of a forensic nasty that had come up in our area.
(04:53) And on the strength of that paper published when I was still a a junior student, um I was invited over to the states and had a go at doing the same thing on black bones collected by Mildred Trotter who was extremely well known for trying to identify bones. Um after the world war I qualified in the [laughter] late 50s, picked up a few desertry prizes and went on to do standard residences, training jobs and so on, including in the clin labs for six months where I frightened myself to death trying to um do emergency tests on all the patients in
(05:32) the hospital who were the most ill. And in those days, us juniors did all the emergency work with no technical help at all after about half a day's training. So you can imagine it was a ferocious introduction to the situation. Anyway, I survived that and went on to get the lecture post that um Jen has mentioned to you uh which was an A+B half with the academic medical unit uh in the university department and half in the national health service.
(06:06) And one of the things I did was go on to set up there assays for the first time in our medical school which is how I got on to vitamin D because obviously uh having seeing patients with ricketetts and osteo Malaysia in our community both in elders and in our dark-kinned immigrants uh we saw a lot of this problem we had to crack on with it [snorts] and one of the really challenging things about working in East London, which I did at the Royal London Hospital, was that we saw a hugely high rate of type 2 diabetes and cardiovascular disease in our um
(06:48) immigrants from Bangladesh. I mean their risk was three to four times as high as those of um our local indigenous people and they also had were notorious for a very high risk of oroparangal cancer. Next slide please. Well, and when we started measuring vitamin D um status, we were totally horrified by how much trouble there was.
(07:18) And we um in the community and we had a trial going on elders with vitamin D which we were trying to measure muscle strength. And one day um during a little break over a cuper, the occupational therapist who was working with us on that came and told me that she had just read something very interesting that um vitamin D replacement if you have deficiency could boost up your insulin secretion to normal.
(07:51) This was an amazing fact to me and I took it on board and wondered if that problem being so common with us might be aggravating more features of the metabolic syndrome and diabetes itself. And I started reading around it, which was why I I wrote up a paper in at the end of the 1990s on whether syndrome X, which we now call metabolic syndrome, was aggravated by deficiency.
(08:22) And yes, virtually every abnormality of metabolic syndrome would increase or decrease according with whether you were deficient or replete. And that was very interesting information. And that's how I came to write this up. At the time, the particular risk factors being investigated back in the '9s were obviously obesity, particularly central, reduced activity, eating horribly high fat intakes.
(08:52) And um it was also suspected that various toxins uh in low dose in the food, particularly nitroso compounds, would increase type two risks. And this had been shown convincingly in animals um not just a few papers but gigantic tomes full of these papers from meetings on it. Um so it was a no-brainer to say to myself, gosh, we have so much type 2 diabetes.
(09:20) Is it all the usual reasons or might this lack of vitamin D which affect your eyelids aggravate the risks? So next slide please. Um so the overall hypothesis therefore was that vitamin D insufficiency would increase the risk of syndrome X as it might be called or metabolic syndrome doesn't matter what you call it the risk of type two.
(09:49) So having been told about this extraordinary new bit of information from the 1980s which it took me about 15 years before I heard it, I started looking into it and it was quite obvious that the variables of the metabolic syndrome would be more abnormal in those who were more deficient and that these seasonal variations in those variables matched those of vitamin D status.
(10:14) So I got quite interested in this and of course vitamin D deficiency was increasingly common globally although it was so easy to correct that it seemed to me worth looking into that being a risk factor for metabolic syndrome because it would be much easier to correct than getting people onto perfect diets with lots of exercise and at their perfect BMI.
(10:39) So let's have the next slide please. Um I this is a sidetracking Eureka moment that I just can't resist. Um privilege of age I think I'll call it. Um it was suddenly reported in the middle of my thinking about these problems that the reason that beetle chewing which is an addictive habit followed by 10% of the world's population 7 million people at the moment um is um the reason that it causes cancer is because the addictive alkoids in the gut when they're acidified by your stomach um they convert into nitrosamines which are carcinogenic.
(11:26) Well, I did a little bit of work on local people and those who chewed this ghastly addictive um chew. Um they we measured their waist size, it was increased the more they chewed and their blood glucoses were higher the more they chewed. And I was asked to talk about those aspects of beetle chewing at a meeting at the International Agency for Research into Cancer, which was about to write up the work of the remarkable Professor Tony Chen, uh, who had been looking at health screening in many hundreds of thousands of people in
(12:03) Taiwan and still increasing numbers. um because and he was able to look at the carcinogenic risks of this habit because in Taiwan the men who chewed didn't add tobacco. So when I was over there there we were sitting down over lunch or something and I said to him rather nervously does your study include any information on blood glucose maybe we could look at that.
(12:32) and he looked at me rather fittingly and said, "Well, of course, we're screening for the five commonest health problems. We've got data for all of it." So, we then published a series of papers showing that the more you chewed and the longer you chewed, the higher the risk of getting not just type two but metabolic syndrome, hypertension and all the other features of metabolic syndrome.
(12:56) And the most interesting thing was because he had huge studies if from the community with family linkage data and their computer services are so good that they could instantly look up the risk to the never chewing descendants of these beetle chewers and rather surprisingly but as with the nitroso compound research in animals those who had never chewed themselves [clears throat] if their par fathers chewed they had an increased risk.
(13:26) So we wrote lots of papers on that and it was interesting. Of course he was interested too in the vitamin D status problem but so far as I know to this day and I met them when they came over a year or so back they have not managed to look at vitamin D status as an added risk factor. Wait for it. It will come. They'll do it in the end.
(13:47) Tony can do anything. Okay. Can we move on past my diversion? Let's go back to the paper that headlines this talk. It's important to consider whether supplementation so as to get rid [clears throat] of deficiency does reduce insulin resistance and whether that has the expected benefits of reducing your risks of type 2 diabetes.
(14:10) So that's what that paper was all about. So let's um have the next slide please. There's all sorts of evidence I shoved in that paper. uh quoted and for example uh we showed um nearly 20 years ago now that low status in cohorts for example in the one that we examined in Nita Faruhi's studies in Cambridge um the 10ear risks of metabolic syndrome were reduced the higher your baseline vitamin D status was and that was very interesting that's the first thing I remember seeing on it and Nita Perui went on um about a bit later to report
(14:56) another cohort that she had exactly the same finding for the risks of type 2 diabetes. So that was interesting and others as you see there and 2018 there was quite a large study showing that 12 years after a decent baseline above 75 nanomals your risk was reduced by 70% of getting type two and then um not so long ago the epic cohort showed just [clears throat] in passing excuse me that it was basic ically the 25 hydroxy D was the vitamin D metabolite that was the most strongly associated with these risks. The other
(15:41) metabolites might be linked to a degree but that was the important one [clears throat] and one might just remember that because it comes up later as an important factor in uh health risks. So next slide please. We also know that um the risks of cardiovascular disease are strongly associated with those of type 2 diabetes.
(16:06) That's more than obvious looking at local populations. But Harold Hemsworth recognized that both conditions were associated with an diminished ability of the tissues to use insulin. In other words, he said insensitivity to it, not just lack of it. although both factors may operate together. Now he presented that at three very famous lectures at the Royal College of Physicians uh the year that the Second World War broke out.
(16:38) But it's an astonishing fact that it took 40 years for those conclusions to be accepted. Now, I like to think that was associated with the outbreak of war getting in the way of this very important fact being appreciated. Or was it just the usual lag as seen for other uh tourisms in Britain that has a nasty habit of of neglecting things? I don't know if other countries do the same.
(17:06) The classic example back in the 1700s was in the British Navy where um one a very observant captain James Lind spotted that where fresh fruit had been provided the awful rate of deaths and bleeding and disability due to acute survey scurvy would would fall. So he did in fact the first randomized control trial ever.
(17:36) He filled one ship up with fresh citrus fruit and neglected another but studied them both equally carefully. I mean the difference in rate the rate of illness and death and disability was huge and immensely important for the navy because people ill with sterling made very bad sailors. So why did it take till 1775 before the British Navy acted on that? I wish I knew.
(18:06) Um but anyway eventually it got acted on and even trials became accepted as respectable. Next slide please. Now um there are various things about how vitamin D works on the tissues um that affect how we look at the findings on people of their vitamin D status in relation to their health problems. For example, I mean, years ago, back in the 80s or 60s even, it was worked out that vitamin D activated in the kidneys circulated around the body and was important for bone and muscle health.
(18:44) Fine. and regulated by calcium and parathone. But in the last 20 years, it's been shown and very convincingly mostly by Martin Herson in his department in the north of England that all the target tissues where vitamin D appears to have important effects, they activate their vitamin D make active calcifform. hormone.
(19:22) It's activated by the concentration of the circulating 25 hydroxyd itself, which I'll call the substrate. And it's downregulated by a a tissue um enzyme that destroys 25D. And parathone has absolutely nothing to do with it. Now, most health workers in my country at least don't seem to know about this and don't seem to appreciate how important it is for understanding um data on vitamin D and health.
(19:52) And you know, we've got good evidence that vitamin D status can protect you against various microbial illnesses, reduce their risks. It it is important for regulating innate and particularly acquired immunity from becoming overactivity. And one of the most important things that's been shown that is carefully neglected by by in Britain at least is the fact that if you're obese, the more obese you are, the less you are able to produce this important substrate in the liver because it stops making 25 hydrox.
(20:31) the [clears throat] 25 hydroxilase enzyme that does that activation. And recently it's been shown that exactly the same thing happens in diabetes. So Edaru's work showed that you need up to three times as much vitamin D orally or to take to have if you are very obese to get a decent blood level that does any protection.
(20:57) And this is the same for diabetes. And another extraordinary fact that popped up um as people got bored with trying to fund trials of vitamin D which are very expensive of course and it became increasingly difficult to ensure that people were taking their daily doses although now we know that they are the most effective. They started using large bolus doses.
(21:22) But there's a problem with really large bololises. They don't work. People, it took a while to find that out. One of the studies that showed this was of um children with severe ricketetts and they gave them these bonus doses and the ricketetts was not healed. And you know the mechanism is now known because of course the body thinks that's too much vitamin D.
(21:47) activates your protective mechanisms and so what you're giving in these huge doses doesn't do much good. Right? Okay. Next slide please. So we need to know if we want to protect communities how long this insulin resistance increase um comes to light before you are at risk of actually getting a type 2 diabetes. a lot of good studies.
(22:14) In a large Japanese study, it was 10 to 20 years people [clears throat] in their late 40s at basan uh before minor increases of glycemia appeared. But they did appear about 10 years before the type two was diagnosed in the White Hole study organized by the um famous Harry Keane who was one of the nicest and most efficient researchers I've ever known in which looked at white and South Asian civil servants in the UK in early middle age and they screened them every five years of the book's tolerance tests there over 8,000 subjects and what he did was plot the
(22:54) trajectories over those years for the increase in insulin resistance and then for the appearance of diabetes. Now insulin resistance began to rise. I can't really show this here. This is not big enough but it is there and 20 years before it developed. But the nasty thing was that the [clears throat] that the insulin resistance rose much faster in the South Asians than in the white subjects.
(23:25) Had I been there at the time, I would probably have said, "For goodness sakes, let's measure their vitamin D status, that may be why the South Asians were in more trouble than the whites because nobody was thinking that way then." And I don't think that's ever been done. Never mind. One day someone might look at it. Let's have the next slide please.
(23:45) [clears throat] So the next obvious question is if deficiency is linked to increases in insulin resistance will supplementation that corrects that deficiency reduce the insulin resistance? Well yes it will. And I would like to just mention a study from New Zealand. Uh the ladies who organized this um von Hurst and Kurt um happened to be in England a few hours after I'd retired and they came to see me about the design of their study.
(24:18) They had a whole group of South Asian women who had normal glucose tolerance but raised insulin resistance and they thought this was something a bit unusual and because they were all D deficient. So they thought well we've seen these hints that vitamin D matters for this type of problem uh we want to design a study.
(24:39) So they came and discussed it and I can remember as we sat there talking about it and saying well I wonder can you measure datus towards the end of the study um they didn't want to because it was difficult and expensive and I don't blame them. I think I was I don't know what I was thinking of. I think I thought they'd better measure it to make sure people were actually taking it and not throwing it away as you know many people might do given medicines they don't know anything about.
(25:07) So they did measure it at the end and the findings are fascinating. I mean this was years ago and they've still quoted all the time including as recently as three months ago in a new study. The deficient women would reduce their insulin resistance strikingly, but only if their 25 hydroxyd had reached above 18 nanomles per liter for at least six months during their study.
(25:34) That's interesting, isn't it? And of course, glycemia in type 2 diabetes can be reduced by reducing insulin resistance even if you don't change your insulin secretion. That was shown quite recently. Well, how does vitamin D reduce this increased insulin resistance? Well, there has been quite a lot of work on that.
(25:59) It's basically through effects of vitamin D on liver, um, muscle and, uh, eyelids. And, uh, I was lucky enough to be able to interest Professor Polong in Hong Kong who was working on various metabolic problems, um, in those tissues in having a look at what vitamin D did um, to them. [clears throat] And we have published three papers um all during my retirement of course had time to do the research when I was retired.
(26:34) What we showed was that you reduced the synthesis of triglycerides in your liver uh if you replace the vitamin D through all sorts of mechanisms which um I hinted at in that little scribble down at the bottom. And um they were also these effects were protective to the eyelets because they would reduce the rein andotensin system over activity which helped to protect them and we produced three papers between 2011 and 16 on that sort of thing and that was really very interesting.
(27:10) So if we go on um can we move on? Thank you. Um if you therefore it would seem to me I mean what I've been looking for ever since um we did that work is whether the rates of type 2 diabetes may fall in Finland over time because they had a most awful problem with deficiency and began food fortification as you probably all know in 2003 it wasn't doing too well.
(27:38) So 10 years later they doubled the fortification in food and virtually abolished deficiency in the bulk of the population although they did supplement high-risisk groups and that they got rid of deficiency even in you know most people weren't taking supplements. So I'm waiting to see type two rates fall in Finland and I keep looking.
(28:02) They're looking at type one rates which are beginning to fall. Who knows? Um, keep your eyes open. It may happen for us to see before too long. People are watching. Next slide, please. What else does vitamin D do? Now, I can't point to this, can I? No. But [laughter] this little slide at the top left there is work done in 1980 by Anthony Norman and others in deficiency looking at eyelet function.
(28:35) This is the work that my occupational therapist came and told me about. Um, now normally the eyelids respond to a rise in your blood glucose by firstly reducing the insulin already there and second that's the little peak on the left at the top there and then by increasing the actual secretion of insulin which is the smooth sort of 5 to 10 minute bulge afterwards.
(28:58) you can see that vitamin D replenishment restored your insulin responses to normal. So I did a study in our horribly deficient um immigrant South Asian populations in Bangladesh and this is the side the picture in the middle shows roughly what we showed. These were very deficient people and on the left we did glucose tolerance tests on all of them.
(29:24) on the left are those who were not at risk of diabetes. And um in the middle here, the lowest group, those are the ones who were at risk. That's their vitamin D status, which was obviously a lot lower than the others. And then if you look at the one um next to that, you can see posts supplementation that their levels did rise, but not to to the normal, which is the line on the side there.
(29:50) This group was incredibly deficient because it was the the year after the eruption of Mount Kinatubo and deficiency across the whole world was appalling and certainly in our immigrant Asians it was appalling. So um what I would like you to look at though in terms of insulin secretion is this slide here that you can see with the two sets of lines going up from left to right.
(30:21) One's C 30 minute ceptide long glucose tolerance. Oh, thank you. That's nice. And the other one is just the insulin secretion. Now, yes, that you can see here it went up. Sure, here it goes up. But what the important thing to look at is that the higher your output of insulin was in the first place when you were supplemented, the better your response.
(30:46) And those who have very poor responses down at the bottom of these lines got very little response at all. So that would say to me and I think to most people that if you can reduce insulin resistance by supplementing people then you should be able to reduce type 2 diabetes risks with the associated heart disease risks. But it would need long-term and sustained repletion to to keep things right.
(31:14) You can't put it right one day and expect it to last 10 years. You've got to go on with it. And of course, what this slide I've just shown you here with the 30 minute responses um being better, the more normal your eyelids were to start with says to me that the earlier you start repletion, the better it is.
(31:37) So um that's my view of what we need to do. Right. Next slide please. Now people in medicine are obsessed with randomized control trials and we have confirmed mechanistic effects that are not being confirmed in trials and you've probably all seen the work published showing why trials are often so lousy. I mean, just to mention a few of them, a lot of them because they're not like medicines, you know, it's all or none.
(32:09) A nutrient will produce an S-shaped curve, and if you supplement them when they're on the flat part of the curve at the top or the bottom, you can't expect much response in whatever you want to look at. And the other thing is particularly in in healthy and wealthy countries perhaps particularly yours America um there were too few deficient people being recruited um for the analysis to be able to show anything much.
(32:37) I mean when Adrien Martin at the London in East London started looking at vitamin D for reducing the risk of upper respiratory tract infections he looked at 25 trials and there was no positive results but he suspected from one he' done that it was there. So he went back, he got the individual data on each participant of the 25 trials and reanalyzed the data and he found that if you looked at those who were deficient at the beginning and not those who weren't, then you could show some benefit in reduction of upper respiratory tract infections. And I hope
(33:17) that like me and all my family um those of you who are now vitamin D replete, yes, you get colds of course, but I bet you don't get as many and you don't get as many secondary infections. I think that work was very convincing and um I'm grateful for it. There we go. Okay. The other thing, of course, is that supplementation may not reach the blood level that you need to achieve what you want to see happen.
(33:46) And um because of these difficulties with trials, if you're going to look at trials, it would make sense to make sure you have a baseline level to show they were deficient and levels going along and certainly at the end or preferably all the way through so that you can keep [laughter] adequate levels all through trials so that the benefits can be um maximized for people.
(34:12) And I'm mention that because I'm going to end with the D2-D reanalysis trial reanalysis for the type two risk reduction and it really matters as you will see. Right, you probably already know but I'm going to say it again. Right, next slide please. Um, I've mentioned already that obesity can increase your requirements for vitamin D to achieve a comparable level to someone who's thin.
(34:38) you might need three times as much and that's the same for diabetes and I don't know any trials I maybe there are some I don't know them where such increases have been given and I wish that they had been done but if they're any more done that must be done if you want to have a chance of getting sensible meaningful results even if they're negative they've got to mean something they got to be correct okay next slide please um I'm now coming to the D2-D trial.
(35:10) This trial set up in America, another of these very expensive trials with best Dson Hughes and Antonio Spitz Adel um showed no reduction in risk of type 2 diabetes in that trial even though a lot of people who were deficient were being given or who was in the study were being given 4,000 units a day, which is quite a nice amount compared with what most trials were giving.
(35:38) But maybe because of all the work that was being published and I would like to think that and so might Bill Grant um they went back to reanalyze their findings by basil and achieved vitamin D status right through the trial and I think this is one of the most useful uh reanalyses of a study that I've seen. I mean it showed considerable um humility to go back and reanalyze it like that.
(36:06) But just look what they found. Your type 2 risks in these all these people have pre-diabetes not actual diabetes were reduced about to 70% if your serum 25 hydroxyd was running at above 100 nanomals [clears throat] per liter throughout the trial which was several years long. And that only happened in the group that were taking 4,000 units a day.
(36:35) Um, and the hazard ratios for type two [clears throat] if your values went above 110 was was49. So there was over a 50% reduction. If you got up to 125 nanomles per liter or more, then your reduction in risk was just over 70%. Just as in the other trial I mentioned a minute ago. Now in Britain at least some health bodies are now acting on those findings and I have seen advice for those with pre-diabetes and deficiency to be given 4,000 units a day.
(37:12) I even have a family member with early rheumatoid who's actually, you know, being given things that lower 25 hydroxilation whose blood levels are being measured and she's being told to increase um, you know, her intake. Britain's learning. We might get there one day. And I have the sort [laughter] of feeling that the need for vitamin D provision may eventually begin to gain traction. I would like to think so.
(37:38) But all those findings that I've talked about strongly suggest to me and I hope and I'm sure they would suggest to most people that adequate supplementation in those up as far as they've got pre-diabetes so long as they've still got eyelet function can reduce the risk of type two. And clearly as this risk starts 10 20 years before it the actual condition appears then the earlier in life you correct your dstatus the better and future trials should also allow for higher needs in obesity and hypoglycemia. So next slide please.
(38:18) The current situation is is for this D status is quite frightening because deficiency is common globally at less than 15 nanomals per liter that won't do much to prevent type two or many other things and the risks of being that at that level can be around 50% or more in many Western countries um 80% in Eastern Europe um or even higher in very hot countries and 10% of all Europeans in a recent study um six years ago had severe deficiency less than 13 animals enough to have muscle trouble and bone trouble and I don't know what else. So we need a
(39:02) major paradigm shift to focus public health action onto nonbony health benefits of vitamin D. I mean, anything else is a sad um reflection on our poor um health education of our population and our professional population who are supposed to be looking after us. So, I've said it before, any further trials must be properly designed.
(39:30) So, let's just finish off. I think I've got one more slide, maybe might be two. Can I have the next one? Yes. Conclusions. Repletion of deficiency reduces insulin resistance. I'm not talking about all the other conditions where it has benefits, but it has known effects on liver and muscle and eyelets themselves. Since obesity and diabetes reduce circulating 25D, it's no surprise that obesity is a big risk factor for type two and it would help if the entire population if their increased requirements were properly met. And
(40:07) adequate vitamin D depletion will also protect and improve your insulin responses to hypoglycemia provided you've still got viable eyelet beta cells that are responsive as in the pre-diabetes. So when I look around at the frequency of this problem and the severity of the conditions associated with deficiency and how easy it would be to solve that problem and I hope all of you are busy doing that for yourselves as many people in Britain are beginning to do or certainly they did during COVID.
(40:44) It seems to me and I hope my view is not too busted that not the correct deficiency of vitamin D at the population level is not just a mistake or poor care it is actually negligent and there might come a time when somebody starts suing somebody and saying it's not just negligent it's criminally ne negligent who am I to say but you know my gut feeling is that we might head that way one day if if we're lucky. Thank you very much.
(41:18) I finished. >> Let's hope that you are right. And you know, I've I've had the honor of having um several of our other vitamin D scientists, including Dr. William Grant and Dr. Dr. Michael Hollik who have also discussed the history of the research of vitamin D and the importance of study design and the outright negligence of the non-action.
(41:44) Um, >> never use that word. How marvelous. I thought I was being daring. [laughter] >> It really is. You know, vitamin D deficiency is so easy to prevent uh and correct and it's it it's we call it the lowest hanging fruit to improve overall population health. It's safe. It's inexpensive. Um it's been proven to be effective.
(42:11) You can especially talking about type 2 diabetes, you know, getting people to change their diet is a lot harder than getting them to take a vitamin D supplement. Um so yes uh ne neglig point the the ge public in this country bought vitamin D like there was no tomorrow during COVID and they emptied the shelves of the shops without medical agreement or approval or anything.
(42:40) But I had I've had people come and talk to me about it and say well I'm taking vitamin D. No problem. I take three a day. And I say yes. Well how much is in them? have the faintest idea. And if they don't know, then how do they know it's enough? And you know, I spend a lot of my time I I obviously I say yes, 4,000 units a day is said to be safe in Britain without seeing a doctor, but provided that your family is not full of kidney stone history or sarcidosis making you unduly sensitive to it.
(43:12) So I mean I take that precaution when I waffle on about this to people. Um but you know I don't I don't don't think our medics do. >> Right. Right. And and to show that 4,000 IU was not enough for what percent of the population in that last study. That really is a big eyeopener for how much vitamin D is actually necessary for a lot of these individuals.
(43:36) percentage with obesity and the percentage with um diabetes which can be quite high as you know and it's rising all the time obesity in the western world I mean if they are deficient to start with then they will be grossly deficient they could need imagine 12,000 units a day to get a normal blood level >> right and and I do want to make a quick note and I'll probably add this note at the beginning when I post this but you're you were referring referring to vitamin D serum levels in nanomles per liter and we usually reference uh them
(44:13) in nanogs per milliliters. So um >> oh no no I I it was a uh you know looking at what you had in the slides I should have considered that but note for next time. Uh so just to mention >> everybody here knows the [laughter] commercial. >> Yes. Yes. Yes. So um for example 100 uh nanom moles per liter is equal to 40 nanogs per milliliter.
(44:40) You take the nanogs per milliliter and multiply by 2.5 to get nanom moles. So um hopefully some of those high numbers weren't uh >> you got nanomles multiply by point4.4 0.4 and you've got mamograms. >> Perfect. >> Okay. >> And and have time for anything. [laughter] I do have some questions for you. Um, and I'm glad that you mentioned uh COVID because the first question was, could vitamin D deficiency combined with conditions like diabetes and high blood pressure have created the perfect storm during the CO 19 pandemic and
(45:19) contributed to higher mortality rates in minority populations? Well, I spent many hours of my life as did others in the field in in bit up and down the country, various medical schools and academic institutions trying to educate the government about this because um you know those who were obese um they're much more at risk of deficiency and they had a much higher mortality if you remember from COVID.
(45:53) And in our country, the people who were so-called BME, you know, black and Asian ethnic minority groups had frightening mortalities um from COVID, particularly if they worked in the health service, which was horrendous. They weren't being given vitamin D. And once more, we made endless efforts to get the government to take that on board.
(46:17) We even had MPs working on it with us. And you know, it didn't happen. The real work on educating the British public didn't come from the health services or public health or the government, you know, it came from the media. Where did I see all that? It was in newspapers reporting it. It was in women's magazines at the dentist.
(46:40) And I was impressed with that because when those things appeared over the next months, as I said, the shelves in the pharmacies and the chemist, the supermarkets cleared of vitamin D. You couldn't find any. And that must have helped. Although I think what people didn't always appreciate was how much they might need to be taking. But anything was better than nothing.
(47:02) If you look at the data from people like Michael Hollik's study of, you know, right across America of the status in the months before the COVID pandemic hit, I mean the the infection rate and the mortality rate was strictly related to the deficiency rates. It could have been avoided an awful lot of it. Yes, a lot of research showing that that correlation between vitamin D serum levels and especially the severity of the COVID infection uh and the mortality. Yeah.
(47:38) And and that is that you know it is great that there was a lot of talk about vitamin D but where a lot of people failed especially a lot of experts is exactly what you mentioned. they they failed to mention how much an individual might need and and uh often >> or often >> and these poor individuals people might I love them went to ask their doctors >> right and so they're just going to say by you or something low like that often and I was teaching on vitamins when I was a medical student I believe it's a bit better my daughter qualified in the
(48:13) late 80s and she got about half an hour on vitamins and knew nothing about it and I do hope it's better now. It needs to be. >> Yeah. Yes. Yes. Hopefully, it will improve soon. All right. I have a a few other questions and I do see that uh we've gotten one submitted, but I'm going to just go in order here.
(48:32) Are there certain challenges that diabetics tend to have with vitamin D conversion pathways or genes that affect vitamin D metabolism and use? And I think that you did kind of touch on that with the liver's job of hydroxilating, but can you just kind of review a little bit? >> The enzyme in the liver that produces the important substrate 25 hydroxyd with which we assess status quite rightly and appropriately because it is the most important factor in how tissues um are supplied with um vitamin D so they can activate it inside themselves and get
(49:09) things right. So those people with diabetes, they they can't activate it as well. I'm not sure that I know why not. I must have another look at whether that's been shown. And of course, there may be other genetic funnies about diabetes that I don't know about um that have been are known long or been published. I mean, they could be there.
(49:31) The important thing, I think, if you've got either of those conditions and you're worried about it, um, if only everybody could do it, um, and you're taking vitamin D, you just check that it's achieving a decent blood level. I mean, for me, I would go for 100 nanomals per liter. Sorry, 40 nanogs per ml. [laughter and gasps] >> Okay.
(49:55) Well, and since that is the question that was submitted, um, what is the recommended blood level for vitamin D and is there any additional benefit at 200 nanomles per liter or 80 nanogs per milliliter? And I know that, you know, at Grassroots Health, our our panel of vitamin D scientists have long recommended a target vitamin D level of 40 to 60 nanogs per milliliter.
(50:19) Um some of them you know we we considered extending that range to 40 to 80 nanogs per milliliter but what is your personal recommendation and do you think there is additional benefit over 80 nanogs per milliter? >> I have a nasty feeling that there probably isn't but I don't know and someone needs to look.
(50:43) I mean, I I would expect there to be because there's a plateau S-shaped curves of effects of of blood levels of vitamins, including D. I would expect there to be a level above which you wouldn't expect most people to get benefit from more. There's no point in stuffing it down, you know, if it isn't going to help.
(51:04) It might have bad effects. I don't know. I mean, it's quite difficult to get vitamin D toxicity. It really is quite difficult. You have to take an awful lot and um or have something like saridosis and be vulnerable. Um and I would think that I would I would like to think I might have levels about 120 140 nanoms per liter round about there but not necessarily any higher unless I find good reasons to want to go higher.
(51:35) That's the best I can do. >> Yeah. And I know you know I have had Dr. Ceero Coimbra on and uh Dr. Richard Chang and and we've talked about this this topic uh and also I believe it's kind of a new concept of vitamin D resistance where you do have certain individuals who might have snips in their genes or polymorphisms that uh affect vitamin D conversion, metabolism and and use.
(52:05) And so those are certain things that might need to be overcome by dosing a little bit higher and achieving higher vitamin D serum levels. And and I know that >> not by routinely huge doses across the population. It's those people who show up as not picking up on on supplementation as they should. If someone looks, they might find they they're in that group. Fair enough.
(52:27) It would be nice to think we might get to detecting them. And until we can actually deal with Joe Public who's deficient as routine, there's not an awful lot of hope that we'll get there. >> Exactly. And and it is different. You know, there are the therapeutic uses of vitamin D such as in the Coinbraber protocol.
(52:45) Um but that's slightly different here. We're we're talking about the general recommendations for public health. >> I'm thinking about public, you know, provision for >> Exactly. [laughter] I appreciate both though. Definitely. Um, so the next question, we know that improving the diet can help prevent type 2 diabetes and metabolic syndrome.
(53:05) Can you please explain what is the relationship between diet and dietary changes and vitamin D levels, if there is one? Is it simply that there is more vitamin D provided in a healthier diet, or is there something else going on? >> I'm not sure that I know all the answers on that one. [clears throat] I mean that if it it is quite important what you eat when you take your vitamin D.
(53:31) I mean people who think they'll take it when they go to bed and they haven't eaten for hours and won't eat for they don't absorb as much as when they take it with a fatty meal which is what I always tell people. Take it with your most fatty meal. I mean if it's butter on your toast or whatever it might be that's when you take your vitamin D.
(53:50) And I've had to tell any number of people it's absorbed better if you take it with fat. Um, you know, I'm not I'm not very well informed on this topic. Um, I I mean, if you're grossly obese, it helps to get your weight down. You will get a better activation uh in the liver to form substrate. And look at how important substrate is.
(54:18) No target tissue can do its thing without adequate substrate and that depends on as far as I know hippatic activation. So yes, that really matters. >> Yeah. And and I would also assume that if you're eating a poor diet, a lot of inflammatory foods that that inflammation in the body is also using up more of the vitamin D or preventing uh some absorption of that vitamin D.
(54:45) and and I'm sure there's many other factors that are contributing but um >> difficult to look at some of those but I'm sure they're all there. [laughter] >> Yes. Yes. I mean there are certainly connections between uh chronic inflammation and metabolic syndrome and and all of that as well. And >> yes >> and diet is a big factor in in inflammation.
(55:11) Um okay so I just have one >> more basketball time. Yeah, I have I have one more question that was submitted, but let let's actually let me just two of the questions that were submitted are quite similar, and I'll read them both together. Um, in the studies, were any vitamin D activators such as magnesium and zinc also supplemented? And what about adding vitamin K2 when taking higher doses of vitamin D for endothelial protection? Do you have any recommendations on any of these co-utrients? I've got no no personal experience working on that, but I'm well aware of
(55:45) the fact that in order for vitamin D to work its best, you know, as efficiently as it can, you do need to be well supplied with magnesium. Not over the top, [clears throat] just, you know, what you should be having, what everyone should be having in an adequate diet. I think the same applies to vitamin K.
(56:04) Um, I mean it does matter if you've not got enough of it, your D doesn't do its effects as well as it should. So, you need those things. Um, but you know, until we can get enough vitamin D into the general population, it's quite difficult to flap about getting these other things right. I just how you tackle it.
(56:28) Unless public health decides to have a go at what's a healthy diet. Generally for a population it's going to take a little time to get there. >> Right. Right. And you know every nutrient where >> Oh sorry >> I'm just saying you're right. Those things do matter. [snorts] >> Yeah. Yes. Of course. And you know there's recommended intakes for all of these nutrients.
(56:50) And yet I know magnesium is one of those that is also severely deficient in terms of intake in our country and likely worldwide. vitamin K2, you need to be, you know, having a lot of fermented foods in your diet. And I don't think that very many people, especially here in the US, are getting enough. Um, and so we like to look at all of the we like to look at how all the nutrients work together as an orchestra, right? We need um optimal intake of all of them.
(57:20) And what sets vitamin D apart? We're meant to get it from the sun, not necessarily from our food. and and here we are sitting inside all day and putting sunscreen on and um so that's what makes >> and babies with four and um you know practically coats hanging off their heads. [laughter] >> Yeah, there's a fear of the sun and we need to overcome that and and its consequences that have resulted in vitamin D deficiency.
(57:49) When I was first a student, people were discovering that, you know, there was an endocrine orchestra headed by the pituitary gland and that this was a a great focus for research, which was quite useful. We need the same thing for vitamins. You know, take it as something that needs doing overall, not just bit by bit. >> Right. Right. I have one last question.
(58:13) Um, and it has to do with fatty liver. So, um I cannot seem to get my vitamin D level up and it is very concerning. I have type 1.5 for 11 years now. I am 59 years of age. I sunbathe uh when there is sunshine and I take vitamin D around 2 to 3,000 daily, which I'm just making an insert here is likely too low.
(58:37) Uh we have always watched vitamin D level in diabetes. I don't know what could be the issue. I am sure I have fatty liver uh but uh and has been gluten-free. Any thoughts? Um and I think maybe just to summarize that question because we've discussed the doses needed and and all that, but could fatty liver also contribute to um a uh lack of dose response to vitamin D? >> Of course.
(59:09) And what's more, if your levels are not quite right, you're more likely to have a fatty liver. And um I would have thought from what I've presented the published data that if you have type one, you're unlikely to have a perfect blood glucose 24/7 every day of the week forever. I mean, it's very very difficult.
(59:31) And if you tend to have a higher sugar on and off, you need more vitamin D. So, why not try increasing your 2 to 3,000 to 4,000 and make sure you're taking it with what fat you eat and see what happens to your blood level. But don't look like tomorrow it may take weeks or some months to see a change. But it will be worth trying. That's what I do.
(59:54) >> Yeah. Right. Well, Barbara, that's it for our questions. Um, did you have anything that you'd like to close with? any additional remarks that um you know before we say goodbye. >> Well, I just to say that I have appreciated the work I've seen coming from your group. I think it's so nice to see a group that looks at things as acceptable to talk about and deal with that in my country our medical and public health people can't be bothered with.
(1:00:25) And you know, I think you're doing a great job and you'll get there. Public health will pick it up in the end. Keep at it. Don't we? [laughter] >> Thank you. And I plan on it for sure. I I absolutely love talking about vitamin D and continuing to learn more about it. I've been with Grassroots Health for 14 years now and there's just still so much that I do not know.
(1:00:48) Um, and it has certainly been fun to learn from all of the world's top, most experienced vitamin D researchers, including yourself. and I really um am very grateful that you joined us today. Thank you. >> Thank you for asking me. I've enjoyed it. Thank you. >> I'm glad [clears throat] all of our technical stuff worked out today.
(1:01:07) [laughter] >> Okay. Good luck for the future. Bye. >> Yes. Thank you. You too. All right. Bye, everybody