Vitamin D did not speed TB recovery when too little was given in a short time - umbrella analysis
Evolution of evidence on vitamin D supplementation in tuberculosis: A comprehensive umbrella review of nine systematic reviews
Journal of Clinical Tuberculosis and Other Mycobacterial Diseases, 2026, https://doi.org/10.1016/j.jctube.2026.100625
Jhosmer Ballena-Caicedo, Lupita Ana Maria Valladolid-Sandoval, Fiorella E. Zuzunaga-Montoya, Víctor Juan Vera-Ponce
Summary by Claude - June 2026
Bottom line: across nine systematic reviews spanning 2009–2022, adding vitamin D to standard tuberculosis treatment did not consistently improve outcomes in unselected patients — and this umbrella review's sharpest contribution is showing why the apparent "growing evidence" is partly an illusion.
The nine reviews (300–2,991 participants each) drew on the same small pool of primary trials: a citation matrix found just 16 unique RCTs behind 64 trial appearances, a corrected covered area of 37.5% — "very high" overlap. So when later reviews echoed earlier ones, that was repetition of shared trials, not independent confirmation. The authors frame this as guarding against an "inflated impression of cumulative certainty."
For the main outcomes, estimates clustered around no effect: sputum culture conversion RR ~1.04–1.05, time-to-conversion HR ~1.04–1.15, and mortality with no significant difference. Doses in the underlying trials ranged enormously — roughly 1,000 to 50,000 IU/day over 8 weeks, mostly high-dose intermittent cholecalciferol — yet no dose-response pattern emerged. Safety was reassuring: hypercalcemia stayed under 2% with no excess over placebo.
Two subgroup signals survived: carriers of the VDR TaqI "tt" genotype (HR 8.09, but based on ~30 patients) and multidrug-resistant TB (RR 2.40, 95% CI 1.11–5.18). GRADE rated both "very low" certainty.
What this does NOT show: it does not prove vitamin D is useless in TB. Heterogeneous dosing, largely unreported achieved 25(OH)D levels, and tiny subgroups leave room for benefit under optimized regimens or in genetically/clinically defined patients. It also says nothing against correcting deficiency for general health — only against prescribing vitamin D purely to speed TB recovery in everyone.
Why these trials may not be a fair test of vitamin D
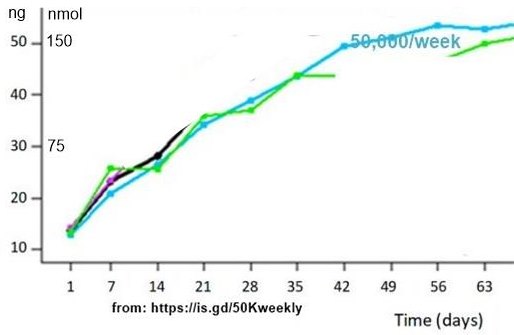
The umbrella review concedes this gap. Most regimens may never have delivered sustained, on-target vitamin D. Daily/weekly dosing (e.g. 50,000 IU/week) takes roughly 5–6 weeks to reach ~40–50 ng/mL and ~11 weeks to plateau — yet the TB trials scored sputum/culture conversion at the end of the same 8-week intensive phase, leaving patients only a couple of weeks actually at an adequate level. The high-dose intermittent (bolus) trials did hit high peaks quickly, but with sawtooth peaks-and-troughs and likely CYP24A1 catabolic upregulation. So a fair reading is that the null reflects inadequate or mistimed dosing as much as true inefficacy — and the untested experiment remains a long-duration, daily, target-confirmed (>40 ng/mL) trial. No commercial sponsor has a reason to run it.
Related in VitaminDWiki
- TB treatment helped by the addition of Vitamin D (100,000 IU bi-weekly) – RCT
- Tuberculosis recovery speeded up by single 450,000 IU dose of vitamin D – RCT
- Tuberculosis -100 percent cure rate with 10,000 IU of vitamin D daily – RCT 2006
- 7100 IU (50000 weekly) got most women to 30 ng of vitamin D
- Weekly 50,000 IU of vitamin D is again found to be good – RCT has the following