Severe COVID-19 not fought by vitamin D when given too late - RCT
📄 Download the PDF from VitaminDWiki
Vitamin D levels increased to avg of 43ng?

All participants appear to have been in hospital a while BEFORE getting Vitamin D
"The mean time between the onset of symptoms and randomization was 10.2 days (SD,4.3);
89.6% required supplemental oxygen at baseline "
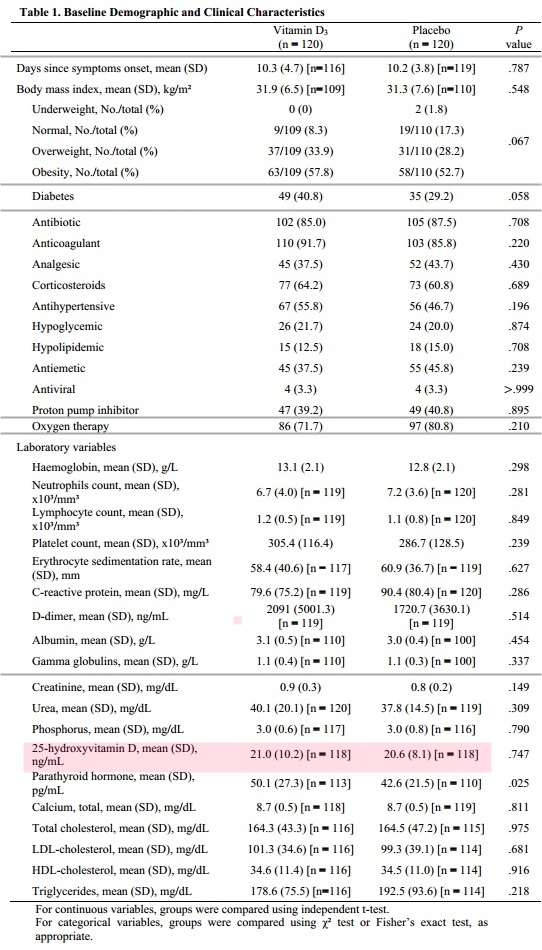
The above is a subset of the table in the PDF
Text and references, but no figures nor tables from the PDF
Effect of Vitamin D3 Supplementation vs Placebo on Hospital Length of Stay in Patients with Severe COVID-19: A Multicenter, Double-blind, Randomized Controlled Trial
Trial Registration: ClinicalTrials.gov Identifier: NCT04449718
Igor H. Murai, PhD; Alan L. Fernandes, PhD; Lucas P. Sales, MSc; Ana J. Pinto, BSc;
Karla F. Goessler, PhD; Camila S. C. Duran, MD; Carla B. R. Silva, MD; Andre S.
Franco, MD; Marina B. Macedo, MD, MSc; Henrique H. H. Dalmolin, MD; Janaina
Baggio, MD; Guilherme G. M. Balbi, MD; Bruna Z. Reis, PhD; Leila Antonangelo,
MD, PhD; Valeria F. Caparbo, PhD; Bruno Gualano, PhD; Rosa M. R. Pereira, MD,
PhD.
Corresponding author (to whom reprint requests should be addressed):
Rosa Maria Rodrigues Pereira, MD, PhD.
Rheumatology Division, Faculdade de Medicina FMUSP, 3° andar, Universidade de
Sao Paulo, Sao Paulo, SP, BR.
Av. Dr. Arnaldo, 455 - Pacaembu - Sao Paulo, SP - Brasil
Postal code: 01246-903. Phone: + 55 11 3061.7490 e-mail: rosamariarp@yahoo.com
Key points:
Question: Can vitamin D3 supplementation reduce hospital length of stay in hospitalized patients with severe COVID-19?
Findings: In this double-blind, randomized, placebo-controlled trial involving 240
hospitalized patients with severe COVID-19, a single dose of 200,000 IU of vitamin D3
supplementation was safe and effective in increasing 25-hydroxyvitamin D levels, but
did not significantly reduce hospital length of stay (hazard ratio, 1.12) or any other
clinically-relevant outcomes compared with placebo.
Meaning: Vitamin D3 supplementation does not confer therapeutic benefits among hospitalized patients with severe COVID-19.
Importance: Patients with COVID-19 may exhibit 25-hydroxyvitamin D deficiency,but the beneficial effects of vitamin D3 supplementation in this disease remain to be proven by randomized controlled trials.
Objective: To investigate the efficacy and safety of vitamin D3 supplementation in
patients with severe COVID-19.
Design, Setting, and Participants: This is a multicenter, double-blind, randomized,
placebo-controlled trial conducted in two centers (a quaternary hospital and a field
hospital) in Sao Paulo, Brazil. The trial included 240 hospitalized patients with severe
COVID-19. The study was conducted from June 2, 2020 to October 7, 2020.
I
nterventions: Patients were randomly allocated (1:1 ratio) to receive either a single
oral dose of 200,000 IU of vitamin D3 or placebo.
Main Outcomes and Measures: The primary outcome was hospital length of stay,
defined as hospital discharge from the date of randomization or death. Secondary
outcomes were mortality, admission to ICU, mechanical ventilation requirement, and
serum levels of 25-hydroxyvitamin D, creatinine, calcium, C-reactive protein, and D-
dimer.
Results: Of 240 randomized patients (mean age, 56 years; 56% men), 232 (96.7%)
were included in the primary analysis. Log-rank test showed that hospital length of stay
was comparable between the vitamin D3 supplementation and placebo groups (7.0 days
[95% CI, 6.1 to 7.9] and 7.0 days [95% CI, 6.2 to 7.8 days]; hazard ratio, 1.12 [95% CI,
0.9 to 1.5]; P = .379; respectively). The rate of mortality (7.0% vs 5.1%; P = .590),
admission to ICU (15.8% vs 21.2%; P = .314), and mechanical ventilation requirement
(7.0% vs 14.4%; P = .090) did not significantly differ between groups. Vitamin D3
supplementation significantly increased serum 25-hydroxyvitamin D levels compared to
placebo (difference, 24.0 ng/mL [95% CI, 21.0% to 26.9%]; P = .001). No adverse
events were observed.
Conclusions and Relevance: Among hospitalized patients with severe COVID-19,
vitamin D3 supplementation was safe and increased 25-hydroxyvitamin D levels, but
did not reduce hospital length of stay or any other relevant outcomes vs placebo. This
trial does not support the use of vitamin D3 supplementation as an adjuvant treatment of
patients with COVID-19.
Introduction
A growing body of evidence has indicated that vitamin D may enhance the innate1-3 and
adaptive immunity.4, 5 Since antigen-presenting cells have the ability to synthesize 1,254 dihydroxyvitamin D (the active form of vitamin D) from 25-hydroxyvitamin D, it has
been postulated that vitamin D supplementation could improve the function of
macrophages and dendritic cells, thereby ameliorating overall immune response.6 In
fact, insufficient vitamin D status has been suggested as a potential risk factor for non-
communicable7 and acute respiratory tract diseases,8, 9 including viral infections.10
In this context, it has been recently conjectured that optimal levels of vitamin D could
play important immunomodulatory and anti-inflammatory roles, thereby benefiting
patients with COVID-19.11, 12 However, the putative benefits of supplementary vitamin
D3 to patients with COVID-19 remain speculative and partially supported by limited
data from observational studies and one small-scale, non-randomized clinical trial.13-15
To our knowledge, this is the first randomized, double-blind, placebo-controlled trial to
investigate the safety and efficacy of vitamin D3 supplementation on hospital length of
stay and other relevant clinical outcomes in hospitalized patients with severe COVID-
- Our main a priori hypothesis was that a single dose of 200,000 IU of vitamin D3
supplementation would increase 25-hydroxyvitamin D levels and shorten hospital
length of stay among these patients.
Methods
The study was approved by the Ethics Committee of Clinical Hospital of the School of
Medicine of the University of Sao Paulo and by the Ethics Committee of Ibirapuera
Field Hospital. All the procedures were conducted in accordance with the Declaration of
Helsinki. The participants provided written informed consent before being enrolled in
the study (Ethics Committee Approval Number 30959620.4.0000.0068). The trial
protocol and statistical plan are included in Supplement 1. This manuscript was written
according to the recommendations by the Consolidated Standards of Reporting Trials
(CONSORT) guidelines (see Supplement 2).
Participants
Hospitalized patients were recruited from Clinical Hospital of the School of Medicine
of the University of Sao Paulo (a quaternary referral teaching hospital), and from
Ibirapuera Field Hospital, both located in Sao Paulo, Brazil. Enrollment started on June
2, 2020, to August 27, 2020, with the final follow-up on October 7, 2020.
Inclusion criteria
Inclusion criteria were: 1) adults aged 18 years or older; 2) diagnosis of COVID-19 by
either polymerase chain reaction (PCR) for severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2) from nasopharyngeal swabs or computed
tomography scan findings (bilateral multifocal ground-glass opacities > 50%)
compatible with the disease; 3) diagnosis of flu syndrome with hospitalization criteria
on hospital admission, presenting respiratory rate > 24 breaths per minute, saturation <
93% on room air or risk factors for complications, such as heart disease, diabetes
mellitus, systemic arterial hypertension, neoplasms, immunosuppression, pulmonary
tuberculosis, and obesity, followed by COVID-19 confirmation before randomization.
Exclusion criteria
Exclusion criteria were: 1) patient unable to read and sign the written informed consent;
2) patient already admitted under invasive mechanical ventilation; 3) previous vitamin
D3 supplementation (> 1000 IU/day); 4) renal failure requiring dialysis or creatinine >
2.0 mg/dL; 5) hypercalcemia defined by total calcium > 10.5 mg/dL; 6) pregnant or
lactating women; and 7) patients with expected hospital discharge in less than 24 hours. 10
Study design and treatment
This was a multicenter, double-blind, parallel-group, randomized placebo-controlled
trial. Eligibility screening was performed between June 2, 2020 to July 21, 2020 at
Clinical Hospital of the School of Medicine of the University of Sao Paulo (n = 122),
and from July 22, 2020 to August 27, 2020 at Ibirapuera Field Hospital (n = 118). The
final follow-up in both centers was on October 7, 2020. Eligible patients were assigned
in a 1:1 ratio into either the vitamin D3 supplementation group or the placebo group.
The randomization list was created using a computer-generated code, which was
managed by a staff member who had no role in the study. We assessed patients5 clinical
status, coexisting chronic diseases, demographic characteristics, self-reported body
weight and height, and ethnicity on hospital admission. Outcomes were assessed at
baseline and on hospital discharge or death records.
The vitamin D3 supplementation group received an oral, single dose of 200,000 IU of
vitamin D3 dissolved in a 10 mL of peanut oil solution on the same day of
randomization. The selected dose is within the recommended range for effectively
promoting vitamin D sufficiency.16 Patients in the placebo group received 10 mL of
peanut oil solution. The vitamin D3 and placebo solutions were identical in color, taste,
smell, consistency, and container. Both were prepared by the pharmacy unit of Clinical
Hospital and labeled by a staff member who did not participate in the study. Allocation
blindness was kept until the final statistical analysis.
Outcome measures
The primary outcome was hospital length of stay, defined as the total number of days
that patients remained hospitalized from the date of study admission until the date of
hospital discharge or death. The criteria used for patient discharge were: 1) no need for
supplemental oxygen in the last 48 hours; 2) no fever in the last 72 hours; and 3)
oxygen saturation > 93% in room air without respiratory distress.
The secondary outcomes were: 1) mortality; 2) number of patients admitted to the
intensive care unit (ICU); 3) number of patients who needed mechanical ventilation and
duration of mechanical ventilation; and 4) serum levels of 25-hydroxyvitamin D
(assessed by a chemiluminescent immunoassay), calcium (assessed by a NM-BAPTA
method), creatinine (assessed by a colorimetric assay based on kinetic Jaffe’s reaction),
and C-reactive protein and D-dimer (both assessed by an immunoturbidimetric assay).
The biochemical analyses were carried out in an accredited laboratory from Clinical
Hospital.
Statistical Analysis
Considering the lack of data available for sample size determination based on the
primary outcome (i.e., hospital length of stay after vitamin D3 supplementation in
patients with severe COVID-19), the number of participants was chosen on the basis of
feasibility, such as resources, capacity of research staff and facility, and available
patients, in line with current recommendations.17, 18 Subsequently, we calculated sample
size assuming a 50% between-group difference in hospital length of stay (considering 7
days as a median time of stay, with an expected variability of 9 days). By considering a
power of 80% and a 2-sided significance level of 5% (a = .05), the total sample was
estimated to be 208 patients (104 in each arm). Considering possible dropouts, and to
increase the power for secondary outcomes, we opted by increasing the sample size by
approximately 15%.
All analyses were carried out following the intention-to-treat principle for all
randomized patients, with no imputation for any missing data. Proportions were
compared between groups using %2 test and Fisher's exact test. Student's t-tests were
used for comparing continuous variables at baseline. The log-rank test was used to
compare the Kaplan-Meier estimate curves the number of days for hospital length of
stay, the primary outcome. Cox regression models for hospital length of stay, admission
to ICU and mechanical ventilation requirement were adjusted by potential confounders
that were not fully balanced by randomization (P < .2) to estimate hazard ratios (HR),
with corresponding 2-sided 95% CI. Generalized estimating equations (GEE) for
repeated measures were used for testing possible differences in laboratory parameters,
assuming group and time as fixed factors, with marginal distribution, and a first-order
autoregressive correlation matrix to test the main and interaction effects. Post-hoc tests
with Bonferroni5s adjustment were performed for multiple comparisons. The
aforementioned statistical procedures were also carried out in post-hoc sensitivity
analyses involving patients exhibiting 25-hydroxyvitamin D deficiency (i.e., < 20
ng/mL).
Statistical analyses were performed with IBM-SPSS software, version 20.0.
Significance level was set at a = .05.
Results
Patients
Of 1208 patients assessed for eligibility, 240 were eligible and randomly assigned to
either the vitamin D3 group or the placebo group. Patients were non-eligible due to the
following reasons: 284 were at ICU, 263 had hospital discharge within 24 hours, 217
did not have COVID-19 confirmation, 95 had renal dysfunction, 37 had dementia or
severe mental confusion hampering their ability to provide the inform consent for
participation, 30 were pregnant or lactating women, 14 had hypercalcemia due to
metastatic neoplasm, 11 were receiving vitamin D3 (> 1000 IU/day), 9 were younger
than 18 years, 6 were illiterate and, therefore, unable to read and sign the informed
consent, and 2 died before randomization.
Of the 120 patients who were randomized to the vitamin D3 group, 3 did not receive
intervention (1 withdrew the consent, 1 vomited immediately after ingesting the
supplement, and 1 was admitted to the ICU before taking vitamin D3) and 3 were lost to
follow-up. Of the 120 patients who were randomized to the placebo group, 2 withdrew
the consent. Thus, of the 240 patients randomized, 232 (96.7%) completed the follow-
up (Figure 1).
Overall, patients5 age was 56.3 years (SD, 14.6), BMI was 31.6 kg/m2 (SD, 7.1), 56.3%
were men, 55% were white, 52.5% had hypertension, 35% had diabetes, 13.3% had
cardiovascular diseases, and 6.3% had asthma. The mean time between the onset of
symptoms and randomization was 10.2 days (SD, 4.3); 89.6% required supplemental
oxygen at baseline (183 were on oxygen therapy and 32 were on non-invasive
ventilation), and 59.6% had computed tomography scan findings suggestive of COVID-
- Demographic and clinical characteristics did not significantly differ between groups,
except for sore throat, which was more prevalent in the vitamin D3 group vs placebo
(38.3% vs 24.2%, P = .026), and PTH, which was higher in the vitamin D3 group vs
placebo (50.1 vs 42.6 pg/mL, P = .025) (Table 1).
Primary Outcome
Hospital length of stay (Figure 2) was comparable between the vitamin D3 group and
the placebo group (7.0 days [95% CI, 6.1 to 7.9] and 7.0 days [95% CI, 6.2 to 7.8 days],
HR, 1.12, [95% CI, 0.9 to 1.5]; P = .379; respectively). The Cox regression model did
not show any significant associations between this outcome and potential confounders.
Secondary Outcomes
There were no significant differences between the vitamin D3 group and the placebo
group for mortality (7.0% vs 5.1%; P = .590), admission to ICU (15.8% vs 21.2%; P =
.314) and mechanical ventilation requirement (7.0% vs 14.4%; P = .090) (Figure 3).
Duration of mechanical ventilation was also comparable between the vitamin D3 group
(18.1 days [95% CI, 3.5 to 32.7]) and the placebo group (11.4 days [95% CI, 7.1 to
15.6]; P = .549, respectively).
The Cox regression model did not show significant associations between secondary
outcomes and potential confounders.
Vitamin D3 supplementation significantly increased 25-hydroxyvitamin D levels vs
placebo (difference, 24.0 ng/mL [95% CI, 21.1- 26.9]; P < .001) (Figure 3). Following
the intervention, 86.7% of the patients in the vitamin D3 group showed 2522 hydroxyvitamin D levels above 30 ng/mL (vs 10.9% in the placebo group), and only 6.7% of the patients in the vitamin D3 group exhibited 25-hydroxyvitamin D deficiency
(vs 51.5% in the placebo group).
Post-hoc Sensitivity Analyses
In a sensitivity analysis involving patients with 25-hydroxyvitamin D deficiency at
baseline (n = 116) (Supplementary Table 1), vitamin D3 supplementation significantly
increased 25-hydroxyvitamin D levels vs placebo (difference, 22.7 ng/mL [95% CI,
19.3 to 26.1]; P < .001) (Figure 3). Among the patients with 25-hydroxyvitamin D
deficiency, no between-group differences were observed in length of hospital stay
(Figure 2). In addition, there were no significant differences between the vitamin D3
group and the placebo group for mortality (7.0% vs 1.7%; P = .206), admission to ICU
(17.5% vs 15.5%; P = .806), and mechanical ventilation requirement (7.0% vs 8.6%; P
.999) (Figure 3). Duration of mechanical ventilation did not differ between the
vitamin D3 group (15.0 days [95% CI, -12.0 to 42.0]) and the placebo group (12.6 days
[95% CI, -7.6 to 26.0]; P = .730).
Safety and Adverse Events
There were no changes in any health-related laboratory markers following the
intervention (Table 2). Vitamin D3 supplementation was well tolerated and no severe
adverse events were reported throughout the trial, with the exception of one patient who
vomited following vitamin D3 administration.
Discussion
This is the first randomized, double-blind, placebo-controlled trial to show that vitamin
D3 supplementation is safe and increases 25-hydroxyvitamin D levels, but is ineffective
to improve hospital length of stay or any other clinical outcomes among hospitalized
patients with severe COVID-19.
Vitamin D has been postulated to play an important role on immune system, acting as a
regulator of both innate and adaptative responses.6, 19 Observational studies have shown
that 25-hydroxyvitamin D levels are associated with better clinical outcomes in
respiratory diseases.20 Positive associations between low 25-hydroxyvitamin D levels
and poor prognosis among patients with COVID-19 have also been observed.21
Furthermore, a small-scale, non-randomized trial demonstrated that the administration
of regular boluses of vitamin D3 before the infection was associated with better survival
and less severe disease among older, frail patients with COVID-19.22 In the current trial,
however, a single dose of 200,000 IU of vitamin D3 supplementation failed to promote
any clinically relevant effects among hospitalized patients with severe COVID-19,
contesting the utility of supplementary vitamin D3 as a treatment in this disease.
The lack of clinical benefits seen in this study was independent of the ability of vitamin
D3 supplementation to increase serum 25-hydroxyvitamin D levels. In fact, following
the intervention, 86.7% of the patients in the supplementation arm achieved vitamin D
sufficiency (> 30 ng/mL) vs 11% only in the placebo group. In a sensitivity analysis
confined to the patients exhibiting 25-hydroxyvitamin D deficiency, vitamin D3
supplementation remained effective in increasing 25-hydroxyvitamin D levels vs
placebo; yet, no clinical improvements were noted. Collectively, these analyses indicate
that a single oral dose of 200,000 IU of supplementation can rapidly increase 2520 hydroxyvitamin levels, in agreement with our hypothesis, so that the present null findings cannot be attributed to the failure of increasing serum 25-hydroxyvitamin D
levels.
Despite the clinical inefficacy of vitamin D3 supplementation, the intervention was not
associated with any important adverse events or meaningful changes in laboratory
parameters, suggesting that a relatively high-dose of vitamin D3 can be well tolerated in
general and free of adverse effects in patients with COVID-19.
The strengths of this study include the randomized, double-blind, placebo-controlled
experimental design, the adequate power, particularly for the primary analysis, the very
low attrition rate (3.3%), the concomitant assessment of 25-hydroxyvitamin D levels
along with clinical outcomes, and the assessment of hospitalized patients with severe
COVID-19.
Limitations
This trial has several limitations. First, the sample size could have been underpowered
to detect significant changes for the secondary outcomes. Second, as the patients had
several coexisting diseases and were subjected to a diverse medication regimen, the
results could have been affected by the heterogeneity of the sample and its treatment.
Third, the proportion of patients with 25-hydroxyvitamin D deficiency enrolled in this
study was considerably lower than those reported in other cohorts,23 possibly as a
consequence of differences in geographic locations. Although we conduced sensitivity
analyses involving patients with 25-hydroxyvitamin D deficiency, one could argue that
they could have been underpowered, as previously pointed out. Therefore, caution
should be exercised in generalizing these findings to patients from other geographical
regions. Finally, the findings should be also confined to the dose and supplementation
strategy used in this trial. Further studies should determine whether preventive or
early vitamin D3 supplementation could be useful in the treatment of patients with COVID-
19, especially those with a mild or moderate disease.
Conclusions
Among hospitalized patients with severe COVID-19, a single dose of 200,000 IU of
vitamin D3 supplementation was safe and increased 25-hydroxyvitamin D levels, but
did not reduce hospital length of stay or any other clinically relevant outcomes vs
placebo. Thus, this trial does not support the use of vitamin D3 supplementation as an
adjuvant treatment of patients with COVID-19.
Article information
Author Affiliations: Rheumatology Division, Hospital das Clinicas HCFMUSP,
Faculdade de Medicina da Universidade de Sao Paulo, Sao Paulo, Brazil (Murai,
Fernandes, Sales, Duran, Silva, Franco, Macedo, Dalmolin, Baggio, Balbi, Reis,
Caparbo, Pereira); Applied Physiology & Nutrition Research Group; Faculdade de
Medicina da Universidade de Sao Paulo, Sao Paulo, Brazil (Pinto, Goessler, Gualano);
Clinical Pathology Division, Hospital das Clinicas HCFMUSP, Faculdade de Medicina
da Universidade de Sao Paulo, Sao Paulo, Brazil (Antonangelo); Food Research Center,
Universidade de Sao Paulo, Sao Paulo, Brazil (Gualano).
Author Contributions: Dr. Pereira had full access to all of the data in the study and
take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Murai, Fernandes, Pinto, Goessler, Gualano, Pereira.
Acquisition, analysis and interpretation: All authors.
Drafting of the manuscript: Murai, Fernandes, Gualano, Pereira.
Critical revision of the manuscript for important intellectual content: AW authors.
Statistical analysis: Murai, Fernandes, Pinto, Reis, Gualano, Pereira.
Obtained funding: Gualano, Pereira.
Supervision: Gualano, Pereira.
Administrative, technical, or material support: Sales, Antonangelo, Caparbo.
Conflict of Interest Disclosures: The authors have nothing to disclose.
Funding/Support: This study was supported by Sao Paulo Research Foundation
(FAPESP) (grants 20/05752-4; 19/24782-4; 20/11102-2; 16/00006-7; 17/13552-2;
15/26937-4; 19/18039-7) and Conselho Nacional de Desenvolvimento Cientifico e
Tecnologico (305556/2017-7).
Data Sharing Statement: See Supplement 3.
Additional Contributions: The authors are thankful to Dr. Monica Pinheiro and Dr.
Roberta Costa for the assistance at Ibirapuera Field Hospital; Dr. Rogerio Ruscitto do
Prado for conducting statistical analyses; Mayara Diniz Santos for the technical support;
all the staff members from both centers; all the patients who participated in this study.
References
Liu PT, Stenger S, Li H, et al. Toll-like receptor triggering of a vitamin D- mediated human antimicrobial response. Science. Mar 2006;311(5768):1770-3. doi:10.1126/science.1123933
Aglipay M, Birken CS, Parkin PC, et al. Effect of High-Dose vs Standard-Dose Wintertime Vitamin D Supplementation on Viral Upper Respiratory Tract Infections in Young Healthy Children. JAMA. Jul 18 2017;318(3):245-254. doi:10.1001/jama.2017.8708
Campbell GR, Spector SA. Autophagy induction by vitamin D inhibits both Mycobacterium tuberculosis and human immunodeficiency virus type 1. Autophagy. Oct 2012;8(10):1523-5. doi:10.4161/auto.21154
van Etten E, Mathieu C. Immunoregulation by 1,25-dihydroxyvitamin D3: basic concepts. J Steroid Biochem Mol Biol. Oct 2005;97(1-2):93-101. doi:10.1016/j.jsbmb.2005.06.002
Laplana M, Royo JL, Fibla J. Vitamin D Receptor polymorphisms and risk of enveloped virus infection: A meta-analysis. Gene. Dec 2018;678:384-394. doi:10.1016/j.gene.2018.08.017
Bilezikian JP, Bikle D, Hewison M, et al. MECHANISMS IN ENDOCRINOLOGY: Vitamin D and COVID-19. Eur J Endocrinol. Nov 2020;183(5):R133-R147. doi:10.1530/EJE-20-0665
Autier P, Boniol M, Pizot C, Mullie P. Vitamin D status and ill health: a systematic review. Lancet Diabetes Endocrinol. Jan 2014;2(1):76-89. doi:10.1016/S2213-8587(13)70165-7
Aibana O, Huang CC, Aboud S, et al. Vitamin D status and risk of incident tuberculosis disease: A nested case-control study, systematic review, and individual- participant data meta-analysis. PLoS Med. 09 2019;16(9):e1002907. doi:10.1371/journal.pmed.1002907
Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. Feb 2017;356:i6583. doi:10.1136/bmj.i6583
Sabetta JR, DePetrillo P, Cipriani RJ, Smardin J, Burns LA, Landry ML. Serum 25- hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS One. Jun 2010;5(6):e11088. doi:10.1371/journal.pone.0011088
Mitchell F. Vitamin-D and COVID-19: do deficient risk a poorer outcome? Lancet Diabetes Endocrinol. 07 2020;8(7):570. doi:10.1016/S2213-8587(20)30183-2
Martineau AR, Forouhi NG. Vitamin D for COVID-19: a case to answer? Lancet Diabetes Endocrinol. Sep 2020;8(9):735-736. doi:10.1016/S2213-8587(20)30268-0
Meltzer DO, Best TJ, Zhang H, Vokes T, Arora V, Solway J. Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results. JAMA Netw Open. 09 2020;3(9):e2019722. doi:10.1001/jamanetworkopen.2020.19722
Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS One.
2020;15(9):e0239252. doi:10.1371/journal.pone.0239252
Ilie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin Exp Res. Jul 2020;32(7):1195-1198. doi:10.1007/s40520-020-01570-8
Kearns MD, Alvarez JA, Tangpricha V. Large, single-dose, oral vitamin D supplementation in adult populations: a systematic review. Endocr Pract. Apr 2014;20(4):341-51. doi:10.4158/EP13265.RA
Bacchetti P. Current sample size conventions: flaws, harms, and alternatives. BMC Med. Mar 2010;8:17. doi:10.1186/1741-7015-8-17
Bacchetti P, McCulloch CE, Segal MR. Simple, defensible sample sizes based on cost efficiency. Biometrics. Jun 2008;64(2):577-85; discussion 586-94. doi:10.1m/j.1541-0420.2008.01004_1.x
Franco AS, Freitas TQ, Bernardo WM, Pereira RMR. Vitamin D supplementation and disease activity in patients with immune-mediated rheumatic diseases: A systematic review and meta-analysis. Medicine (Baltimore). Jun 2017;96(23):e7024. doi:10.1097/MD.0000000000007024
Cannell JJ, Vieth R, Umhau JC, et al. Epidemic influenza and vitamin D. Epidemiol Infect. Dec 2006;134(6):1129-40. doi:10.1017/S0950268806007175
Carpagnano GE, Di Lecce V, Quaranta VN, et al. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest. Aug 2020;doi:10.1007/s40618-020-01370-x
Annweiler G, Corvaisier M, Gautier J, et al. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients. Nov 2020;12(11)doi:10.3390/nu12113377
Hernandez JL, Nan D, Fernandez-Ayala M, et al. Vitamin D Status in Hospitalized Patients With SARS-CoV-2 Infection. The Journal of Clinical Endocrinology & Metabolism. 2020;doi:10.1210/clinem/dgaa733