RCTs should use individual vitamin D dosing to reach a preset level.
Why did we end up having so few vitamin D answers and what can we do about it? A provocative and narrative review
The Journal of Steroid Biochemistry and Molecular Biology Volume 256, February 2026, https://doi.org/10.1016/j.jsbmb.2025.106895
Rolf Jorde
Highlights
• Guidelines on vitamin D intake are based on questionable studies.
• We do not know what is a sufficient serum 25-hydroxyvitamin D (25OHD) level.
• New vitamin D RCTs should include subjects with low 25OHD levels.
• RCTs should use individual vitamin D dose to reach a preset 25OHD level.
• A consensus conference on how to perform vitamin D RCTs is highly needed
In spite of numerous vitamin D publications, including thousands of RCTs, meta-analyses, review papers and editorials, we still do not have answers to the most basic vitamin D questions. The recommendations for vitamin D intake are based on a few and questionable studies, and according to the latest Endocrine Society Guidelines from 2024, there is no clinical trial evidence for establishing serum 25-hydroxyvitamin D (25OHD) thresholds to define vitamin D deficiency. Furthermore, large and impressive vitamin D RCTs, some with more than 20,000 participants, have failed to show significant effects on disease prevention. However, there are indications that vitamin D may have a small preventive effect on type 2 diabetes and auto-immune diseases, and vitamin D may also improve cancer survival.
In general, the RCTs have been under-powered, and most subjects included were already vitamin D sufficient. The time for new vitamin D mega trials is probably over, and in the future, we have to design our RCTs smarter. One should mainly include subjects with low serum 25OHD levels, use individual dosing to reach a preset 25OHD level [treat-to-target), use realistic power calculations, and we should use similar study designs to facilitate individual patient data meta-analyses. We must be willing to realize that we have failed, we must be willing to change, and we must be willing to pull our forces together. A vitamin D consensus conference is highly needed. We cannot accept that in 2025 we do not know what is a sufficient serum 25OHD level.
RCT Guielines (from PDF)
- To increase chances of a positive result, only include subjects with low baseline serum 25OHD, preferably in the range 30 - 40 nmol/L.
- Treat-to-target. Ideally two targets should be set, one close to the assumed threshold (like serum 25OHD 50 nmol/L) and one higher like 80 nmol/L.
- If treat-to-target is impossible, like in an add-on-study in cancer treatment, use 3000 IU per day. This is a safe dose and will in most subject increase serum 25OHD sufficiently. The use of different doses will, even if all show a positive effect, make results more difficult to implement in clinical practice. This was one of the reasons why the American Diabetes Organization (ADA) did not endorse vitamin D supplementation in prediabetes [25].
- Include subjects at risk of the disease in question, like subjects with prediabetes if want to see effect on diabetes prevention, subjects with positive thyroid antisera (anti-TPO) if want to prevent hypothyroidism and so on.
- Focus on conditions where previous studies most strongly have indicated a positive effect of vitamin D like prediabetes [9], pregnancy [9], mortality [9], cancer survival [2], and autoimmune diseases [26].
- Use daily doses of vitamin D (cholecalciferol). Intermittent high doses should be avoided [9].
- VitaminDWiki disagrees
- Use realistic power calculations. The effect looking for is most likely very small. If one cannot include a sufficient number, collaborate with others, or do not do the study.
- Use 25OHD as measure of vitamin D status which is widely accepted. Other measures like free 25OHD or various ratios may be of theoretical interest but has to be evaluated against a gold standard (known levels of vitamin D status) that do not exist.
- Serum 25OHD should be measured with an LC-MS/MS assay which today is the gold standard. Serum samples should be kept for re-analyses if results are questioned.
- Include stratification for BMI in the protocol since for unknown reasons vitamin D effects might be BMI related [21].
- Include stratification for race/ethnicity since the vitamin D response for some outcomes may be race dependent [2].
- The length of the intervention should depend on the outcome. For outcomes where subjects at risk can be identified (prediabetes, auto-antibodies), the intervention period should be five years. For outcomes like cancer, where subjects at risk are hard to identify, the intervention period should be longer, preferably 10 years.
- If the RCT is long lasting, continue follow-up for at least one year since the vitamin D group will have higher serum 25OHD for a prolonged time [17,27].*
Related in VitaminDWiki
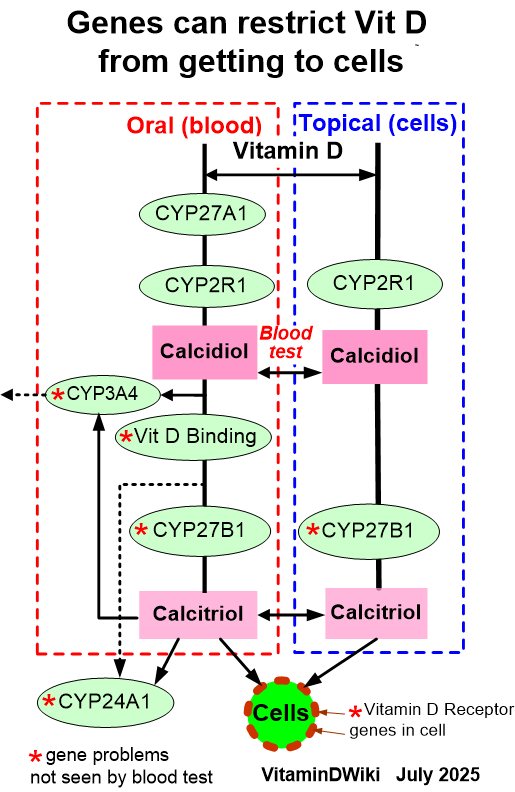
- Vitamin D non-responders may have one or more poor genes: GC, LIPC, CYP24A1, and PDE3B
- No response to Vitamin D was 11 X more likely to have if poor Binding gene
- Poor responses to UV and Vitamin D were correlated to just 4 poor genes
Response to Vitamin D fortification varies from 1 to 10 nmol per 100 IU daily – review Aug 2023
No response to vitamin D 7X more likely if poor CYP24A1 or VDBP genes - Feb 2023
Molecular Approaches for Optimizing Vitamin D (one size does not fit all) – Carlberg Nov 2015
Vitamin D Nutrigenomics - High, Medium, and Low Responders - March 2019
- Gut-Friendly Vitamin D
- Vitamin D and Liposomal Glutathione restore the immune system
- Glutathione improves Vitamin D in 9 ways
- Genetics: most Vitamin D genes are not noticed by Vit D test