Gut, microbiome, and Vitamin D - Narrative book chapter
The Vitamin D- Microbiome Axis: Mechanistic Insights into Gut
Immunity and Health
Asked Claude AI:
Please summarize this PDF and indicate where it agrees or disagrees with other publications
Selvakumar & Jagal (IntechOpen 2025, Univ. of Sharjah) is a narrative book chapter, not a systematic review. It organizes the vitamin D–gut literature into five mechanistic blocks plus a clinical/translational block:
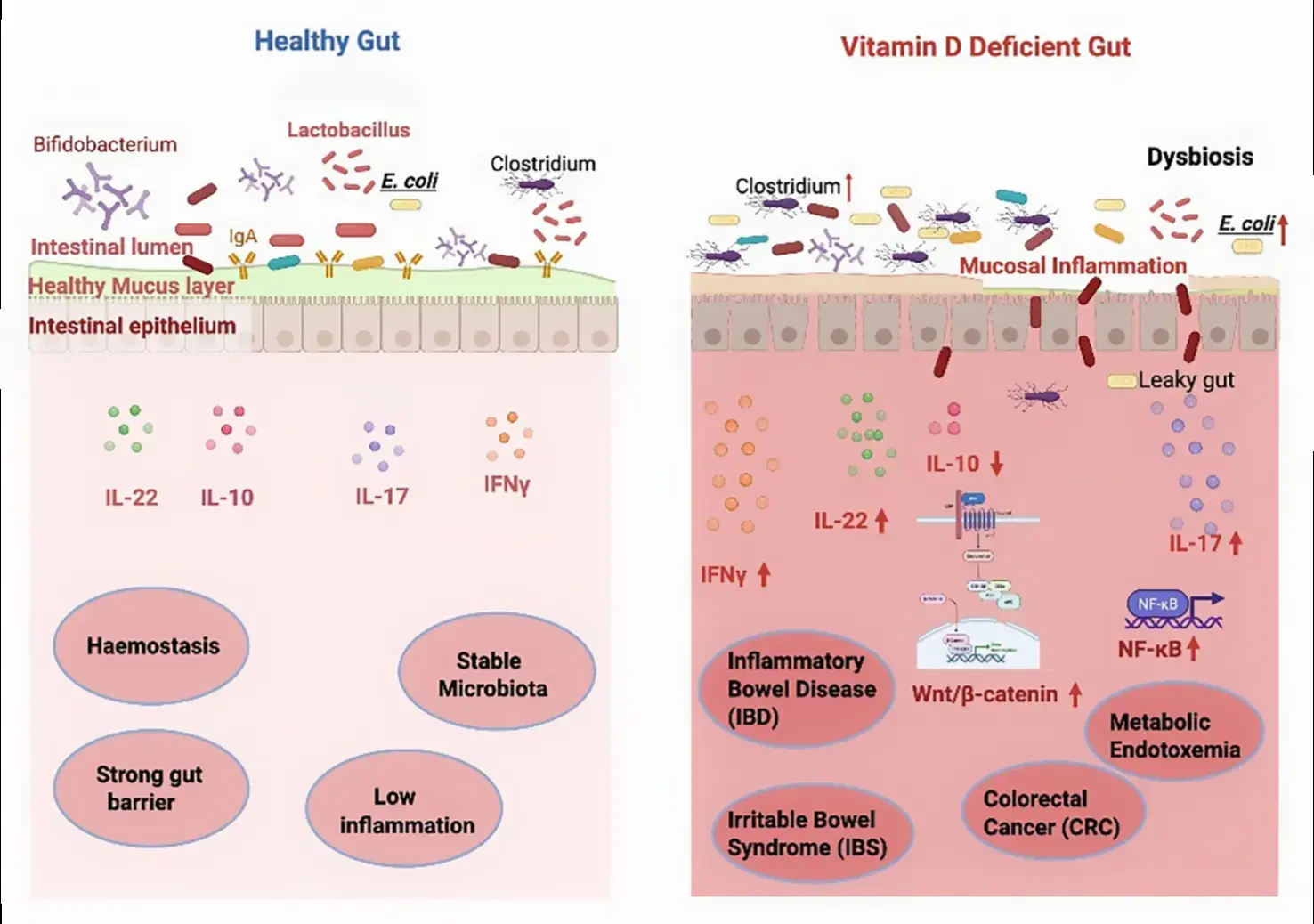
Barrier function. VDR signaling upregulates occludin and stabilizes ZO-1 at the apical junctional complex; tunes specific claudins; reduces paracellular leak; promotes restitution after injury via growth-factor pathways and AMP induction.
Microbiota. VDR shapes the luminal niche indirectly (AMPs, mucin, barrier), favoring Lactobacillus and Bifidobacterium and restraining Enterobacteriaceae; deficiency tracks with reduced diversity and a shift in the Firmicutes/Bacteroidetes ratio; sufficiency supports SCFA-producing taxa and amplifies SCFA action via GPR41/43 and HDAC inhibition.
Innate defense. Direct VDRE-driven induction of cathelicidin (CAMP/LL-37) and β-defensins; preserved Paneth cell function (α-defensins, lysozyme, RegIIIγ); thicker MUC2 mucus; tolerogenic dendritic cells, M2-polarized macrophages, IL-22 from ILC3s, and a TLR↔VDR feed-forward loop.
Adaptive immunity. Suppression of RORγt/Th17, expansion and stabilization of FoxP3⁺ Tregs, tolerogenic DCs (low CD80/86, high IL-10, low IL-12), and reinforcement of oral tolerance in mesenteric nodes.
Clinical. IBD, IBS, CRC, and metabolic endotoxemia all framed as benefiting from keeping 25(OH)D >30–40 ng/mL; dosing examples cited are 2,000 IU/day (12 weeks, IBD), 5,000 IU/day (24 weeks, Crohn's), and 50,000 IU/week (~7,000 IU/day, 6–9 weeks, IBS).
Menopause coda. A late, somewhat off-topic section on estrogen–VDR crosstalk, the estrobolome, and the case for tailored postmenopausal supplementation.
Where it aligns with the broader literature
The mechanistic core is well-supported and uncontroversial: the cathelicidin VDRE, VDR control of tight junctions, Th17/Treg modulation, and tolerogenic DC induction are all consistent with Cantorna's group, Sun's group, Hewison/Bishop, and the Fakhoury 2020 review the chapter cites. The IBD framing matches recent meta-analytic evidence — Valvano et al. (2024, Inflamm Bowel Dis) found vitamin D supplementation reduced clinical relapse risk in IBD overall (RR 0.64) and especially in Crohn's in remission (RR 0.47), and Dell'Anna et al. (2025, Nutrients, which the chapter cites as ref 67) tied low 25(OH)D to higher disease activity, mucosal inflammation, lower QoL, and relapse across 27 studies / 8,316 patients. The 30 ng/mL threshold target is consistent with the IBD-specific consensus.
Where it disagrees with, or oversimplifies, the literature
Menopause timing — this is the most clearly wrong claim. The chapter states that "postmenopausal women with Vitamin D deficiency (<20 ng/mL) experienced delayed menopause" (citing Muho 2025). The prevailing evidence runs the other direction. NHANES 2001–2018 (n=6,326) found vitamin D deficiency associated with earlier menopause and shorter reproductive lifespan, and the Nurses' Health Study II prospective cohort (1.13 million person-years) linked higher vitamin D intake to lower risk of early menopause. The Sister Study (mean baseline age 46) found no association either way. Either Muho 2025 is an outlier in a small cohort, or the chapter has summarized it incorrectly; in either case the statement should not be taken at face value.
Firmicutes/Bacteroidetes ratio as a "key marker of gut microbial health." Magne et al. (2020, Nutrients) and subsequent work have argued this ratio is not a robust dysbiosis biomarker — discrepancies across studies reflect methodology and population heterogeneity more than biology. The chapter presents it as settled. Modern reviews increasingly look at specific taxa (Faecalibacterium prausnitzii, Akkermansia muciniphila, Roseburia) and functional capacity rather than the F/B ratio.
"70% of immune cells in GALT." Widely cited but, as a precise figure, more shorthand than census. Some sources estimate up to 70% of lymphocytes — not "immune cells" broadly — reside in the gut. Not wrong enough to flag in a chapter, but worth knowing the figure is rhetorical.
Dosing recommendations are conservative and inconsistent with the threshold logic the chapter itself advocates. The chapter targets >30–40 ng/mL but cites 2,000 IU/day as the IBD adult example — a dose that on average produces a ~10–15 ng/mL rise and routinely leaves heavier or malabsorbing IBD patients below threshold. Higher pulse-loading protocols (e.g., Coimbra-style loading, calcifediol, or weight-based dosing as in the Kojecky 2020 RCT it cites as ref 52) are not foregrounded, and the chapter does not discuss faster-onset metabolites (calcifediol) at all — a notable omission given the role of acute gut-barrier rescue in sepsis/endotoxemia, which it does discuss in mechanism.
Metabolic endotoxemia section is thinner than the mechanism warrants. It correctly cites Lee & Campbell (2009) and Oku 2023 but does not engage with the larger LPS/TLR4/NF-κB intervention trials, nor with the question of whether vitamin D's effect is mediated more through barrier tightening or through direct TLR4 suppression — an active debate.
Notable omissions
The chapter does not address:
- (1) the calcifediol vs. cholecalciferol onset-time question, which matters in acute gut injury;
- (2) the divergent sepsis trials (VITdAL-ICU showed benefit in deficient subgroups; VIOLET did not), even though metabolic endotoxemia is a section heading;
- (3) VDR polymorphism heterogeneity beyond a passing mention in CRC;
- (4) the gap between mechanistic evidence and routine clinical adoption — the research-to-practice tail that's central to your VitaminDWiki framing; and
- (5) population-level deficiency prevalence and the disparities angle (Black, Indigenous, elderly, institutionalized), where the gut-immune story has the strongest potential public-health payoff.
Bottom line for VitaminDWiki use
The mechanistic sections are sound and well-organized — usable as citations for tight junction, AMP, Th17/Treg, and dendritic cell pages, with the Sun 2022 and Fakhoury 2020 references being the strongest in their reference list. Treat the menopause-timing claim as suspect until you check Muho 2025 directly. Treat the F/B ratio framing as outdated. The dosing examples are too low to match the threshold target the chapter itself promotes — a familiar pattern in this literature that's worth flagging when you summarize it.
Related in VitaminDWiki
- Vitamin D improves the Gut Microbiota - review
- Microplastics change the gut microbiome
- Vitamin D levels change Gut Microbiota – 25 study review
- Microbiome
- Microbiome improvement by probiotics can be augmented with phages (gut, etc.)
- Gut Microbiota: improved by Vitamin D – narrative review
- Vitamin D helped by helping gut - German interview, English voiceover
- Vitamin D, Microbiome, Gut Health - Dr. Beltran
- Diarrhea and Vitamin D - many studies
- Irritable Bowel Syndrome and Vitamin D - many studies
- Ulcerative Colitis and Vitamin D - many studies
- Vitamin D and Liposomal Glutathione restore the immune system
- Over 200 immune articles in VDW have Vitamin in the title
- Vitamins and Metals needed by the Immune System