Fewer liver problems (NAFLD, MASLD) if higher Vitamin D -Dec 2025
Association between serum vitamin D levels and metabolic dysfunction-associated steatotic liver disease: a cross-sectional study based on NHANES 2021-2023
Ann Med Surg (Lond). 2025 Oct 14;87(12):8099-8107. doi: 10.1097/MS9.0000000000004048
Shuo Zhou 1 2, Xiao You 2, Dengyong Zhang 2, Song Yang 2, Yongliang Chen 1 3, Wanliang Sun 2
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) is a growing global health concern, and emerging evidence suggests a potential role of vitamin D in its pathogenesis. This study aims to evaluate the impact of serum vitamin D levels on the risk of MASLD using National Health and Nutrition Examination Survey (NHANES) data.
Methods: We analyzed data from 3249 US adults based on NHANES 2021-2023 cycle. MASLD was defined by controlled attenuation parameter value ≥248 dB/m. Three multivariable logistic regression models were constructed: Model 1 (vitamin D alone), Model 2 (partially adjusted), and Model 3 (fully adjusted for demographic, metabolic, and inflammatory factors). Model performance was assessed using receiver operating characteristic analysis, calibration curves, and decision curve analysis (DCA). The mediation analysis was used to explore these associations.
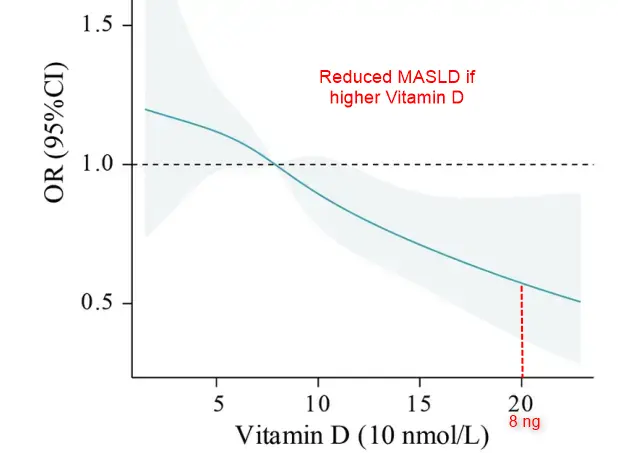
Results: The analysis revealed that the MASLD group had significantly lower median vitamin D levels (77.35 vs. 82.10 nmol/L, P < 0.001) and a higher percentage in the lowest vitamin D quartile (27.2% vs. 22.1%, P < 0.001). The multivariable logistic regression demonstrated an inverse association between vitamin D and MASLD prevalence, with each 10 nmol/L increase correlating with a 3.5% reduction in MASLD risk [odds ratio (OR) 0.965, 95% confidence interval (CI) 0.941, 0.989, P = 0.005]. Restricted cubic splines confirmed a linear dose-response relationship (P nonlinear = 0.915). The fully adjusted model 3 showed excellent discrimination (AUC 0.825, 95% CI 0.811, 0.839), indicating excellent predictive performance for MASLD risk assessment. DCA further established that the fully adjusted model provided clinically meaningful net benefits across a wide threshold probability range (15-90%) and prevented 38-42% of unnecessary interventions for MASLD management. Mediation analysis indicated that body mass index, high-density lipoprotein cholesterol, and glycohemoglobin mediated 52.11, 19.12, and 6.95% of the association of vitamin D and MASLD.
Conclusions: Our findings suggest that higher vitamin D levels were associated with lower odds of MASLD, highlighting its potential as a modifiable risk factor and a promising therapeutic target.
Transition from NAFLD to MASLD (brief overview) Perplexity AI Dec 2025
Why the change:
NAFLD was defined negatively (fatty liver in people who do not drink “too much” alcohol). This definition:- Centered on alcohol exclusion rather than the positive presence of metabolic risk.
- Stigmatized patients by framing them around “non‑alcoholic.”
- Failed to explicitly tie the condition to metabolic dysfunction.
What MASLD emphasizes:
MASLD is defined as:- Hepatic steatosis on imaging or histology
- Plus at least one metabolic risk factor (e.g., obesity, type 2 diabetes, insulin resistance, dyslipidemia, hypertension). Alcohol is no longer the primary gatekeeper; instead, metabolic dysfunction is central.
Terminology changes within the spectrum:
- NAFLD → MASLD (steatosis with metabolic dysfunction)
- NASH (Non‑Alcoholic Steatohepatitis) → MASH (Metabolic dysfunction–Associated Steatohepatitis)
The pathobiology (steatosis → steatohepatitis → fibrosis → cirrhosis/HCC) remains the same; only naming and criteria shift.
Clinical impact:
- Better alignment with the dominant drivers: insulin resistance, obesity, type 2 diabetes, metabolic syndrome.
- Broader recognition that MASLD is a multisystem metabolic disease (linked to CVD, CKD, etc.), not just a liver condition.
- Some patients previously labeled NAFLD may now be reclassified depending on metabolic criteria and alcohol patterns (e.g., “MetALD” category for mixed metabolic and alcohol‑related disease).
In short: the transition to MASLD reframes “fatty liver” as a metabolic syndrome–driven steatotic liver disease and replaces an exclusionary, alcohol‑based label with a positive, metabolically defined one.