Exercise reduces cancer deaths, Magnesium RDA reduces deaths even more
Physical activity, dietary calcium to magnesium intake, and mortality in the National Health and Examination Survey 1999–2006 cohort
International Journal of Cancer https://doi.org/10.1002/ijc.32634
Elizabeth A. Hibler PhD, MPH Xiangzhu Zhu MD, MPH Martha J. Shrubsole PhD Lifang Hou MD, PhD Qi Dai MD, PhD
 click on chart for details
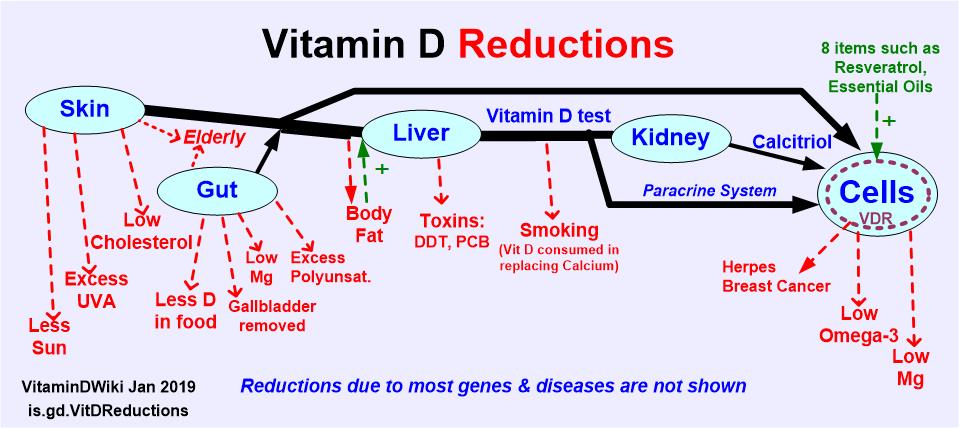
Magnesium is vital to Vitamin D in 4 places (maybe 8) – March 2018
1. Magnesium and Vitamin D contains the following summary
{include}
Overview Magnesium and vitamin D Has a venn diagram of relationship of Mg and Vit D
{include}
click on chart for details
Magnesium is vital to Vitamin D in 4 places (maybe 8) – March 2018
1. Magnesium and Vitamin D contains the following summary
{include}
Overview Magnesium and vitamin D Has a venn diagram of relationship of Mg and Vit D
{include}
📄 Download the PDF from VitaminDWiki
Calcium and magnesium affect muscle mass and function. Magnesium and calcium are also important for optimal vitamin D status. Vitamin D status modifies the associations between physical activity and risk of incident cardiovascular disease (CVD) and CVD mortality. However, no study examined whether levels of magnesium and calcium and the ratio of dietary calcium to magnesium (Ca:Mg) intake modify the relationship between physical activity and mortality. We included 20,295 National Health and Nutrition Examination Survey participants (1999–2006) aged >20 years with complete dietary, physical activity, and mortality data (2,663 deaths). We assessed physical activity based on public health guidelines and sex‐specific tertiles of MET‐minutes/week. We used Cox proportional hazards models adjusted for potential confounding factors and stratified by the intakes of magnesium, calcium, Ca:Mg ratio.
We found higher physical activity was significantly associated with reduced risk of total mortality and cause‐specific mortality, regardless of Ca:Mg ratio, magnesium or calcium intake. In contrast, both moderate and high physical activity were significantly associated with substantially reduced risks of mortality due to cancer when magnesium intake was above the RDA level. We also found higher physical activity was significantly associated with a reduced risk of mortality due to cancer only when Ca:Mg ratios were between 1.7–2.6, although the interaction was not significant. Overall, dietary magnesium and, potentially, the Ca:Mg ratio modify the relationship between physical activity and cause‐specific mortality. Further study is important to understand the modifying effects of the balance between calcium and magnesium intake on physical activity for chronic disease prevention.