Cystic Fibrosis probably treated by Vitamin D (if use enough of the right type )
Vitamin D deficiency and its treatment in cystic fibrosis.
J Cyst Fibros. 2019 Oct;18 Suppl 2:S66-S73. doi: 10.1016/j.jcf.2019.08.022.
Cystic Fibrosis and Vitamin D review with 2012 Guidelines - Nov 2019
Liposomal is better than standard Vitamin D in 10 ways great for poor fat absorption
Vitamin D has been recommended for Cystic Fibrosis – a small dose helps a little – Aug 2018
- Cystic Fibrosis guidelines for Australia include Vitamin D – June 2019
- Cystic Fibrosis exacerbation reduced by Vitamin D (250,000 IU) – RCT May 2017
- Review of Cystic Fibrosis and Vitamin D PDF file, not web page: has the following
- Cystic Fibrosis category listing has items along with related searches
- "Cost of conventional Cystic Fibrosis tratment is $16,000/year"
- it will be a while until the doctors are willing to lose money with Vitamin D and/or Omgea-3**
- Cystic Fibrosis not helped by 50,000 IU of Vitamin D taken twice a month – RCT Feb 2019
- 50,000 IU every 2 weeks raised blood levels by only a tiny amount (~5 ng/ml)
- Clearly the type of vitamin D used was not getting into the blood stream, and so provided very little help Better types of Vitamin D are sometimes needed
- Overview Gut and vitamin D contains gut-friendly information
- |Inhaled Vitamin D
- Powder-based Vitamin D may be gut-friendly (Cystic Fibrosis) – RCT Aug 2017
- Topical Vitamin D provides more benefits than oral sometimes - many studies - as of Oct 2019:: Preeclampsia. Food Allergy, PTSD, Ear infection, Infertility, MS, Colon Cancer, TB, Asthma, COPD, Epilepsy, Atrial Fibrillation. Liver, Also suspect for those people with poor guts: Cystic Fibrosis , Diabetes Omega-3 also helps
- Cystic fibrosis problems cut in half by Omega-3 – RCT June 2015 Vitamin D may also PREVENT Cystic Fibrosis
- Cystic Fibrosis may be related to low Vitamin D – Aug 2017
- If vitamin D levels are less than 40 ng some children get cystic fibrosis – March 2018
Daley T1, Hughan K2, Rayas M3, Kelly A4, Tangpricha V5.
1 Division of Pediatric Endocrinology and Metabolism, Emory + Children's Pediatric Institute, Department of Pediatrics, Emory University, School of Medicine, 1400 Tullie Road, Atlanta, GA 30329, USA. Electronic address: Tanicia.daley@emory.edu.
2 Division of Pediatric Endocrinology and Diabetes, UPMC Children's Hospital of Pittsburgh, University of Pittsburgh School of Medicine, 4401 Penn Avenue, Pittsburgh, PA 15224, USA. Electronic address: kara.hughan@chp.edu.
3 Division of Pediatric Endocrinology and Diabetes, University of Texas Health San Antonio, 7703 Floyd Curl, San Antonio, TX 78229, USA. Electronic address: rayas@uthscsa.edu.
4 Division of Pediatric Endocrinology and Diabetes, Children's Hospital of Philadelphia, Perelman School of Medicine of University of Pennsylvania, 2716 South Street, Philadelphia, PA 19146, USA. Electronic address: kellya@email.chop.edu.
5 Atlanta VA Medical Center, 1670 Clairmont Road NE, Decatur, GA 30300, USA; Division of Endocrinology, Metabolism, and Lipids, Department of Medicine, Emory University, School of Medicine, 101 Woodruff Circle NE, Atlanta, GA 30322, USA. Electronic address: vin.tangpricha@emory.edu.
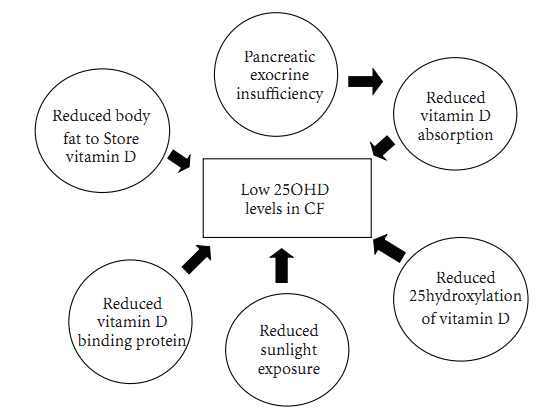
Vitamin D deficiency is a common finding in individuals with cystic fibrosis (CF), despite routine supplementation. Hypovitaminosis D is often the result of fat malabsorption, but other contributors include increased latitude, poor nutritional intake, decreased sun exposure, impaired hydroxylation of vitamin D, and non-adherence to the prescribed vitamin D regimen. Vitamin D is critical for calcium homeostasis and optimal skeletal health, and vitamin D deficiency in CF can lead to skeletal complications of osteopenia and osteoporosis.
Over time, our understanding of treatment regimens for vitamin D deficiency in CF has evolved, leading to recommendations for higher doses of vitamin D to achieve target levels of circulating 25-hydroxyvitamin D.
There is also some evidence that vitamin D deficiency may have non-skeletal consequences such as an increase in pulmonary exacerbations.
The exact mechanisms involved in the non-skeletal complications of vitamin D deficiency are not clearly understood, but may involve the innate immune system. Future clinical studies are needed to help address whether vitamin D has a role in CF beyond skeletal health.