5 Critical Analyses of the 2024 Endocrine Society Guideline on Vitamin D
Summary
Pilz et al. (Nutrients, May 2026) provide a comprehensive summary and critical appraisal of the 2024 Endocrine Society Clinical Practice Guideline on vitamin D (Demay et al., JCEM 2024). The Endocrine Society guideline — built on GRADE + Evidence-to-Decision methodology with RCT priority — recommends empiric vitamin D supplementation (above DRI, without 25(OH)D testing) for four populations only:
| Population | Indication | Trial weighted avg | Trial range |
|---|---|---|---|
| Ages 1–18 | Rickets, RTIs | ~1,200 IU/d | 300–2,000 IU |
| Ages ≥75 | Mortality | ~900 IU/d | 400–3,333 IU |
| Pregnancy | Preeclampsia, IUM, preterm, SGA, neonatal mortality | 2,500 IU/d | 600–5,000 IU |
| Prediabetes (high-risk) | T2DM progression | ~3,500 IU/d | 842–7,543 IU |
Key methodological positions of the guideline: against routine 25(OH)D screening (including in dark skin and obesity); 30 ng/mL threshold from 2011 abandoned; daily over intermittent dosing for ≥50; healthy 50–74 may rationally choose to supplement; and — per a 2025 correction — the 2024 guideline replaces the 2011 guideline.
Pilz et al. organize their critique into six domains: dose uncertainty, target-population gaps, implementation, laboratory testing, new evidence, and outlook (sun/UV-B).
Where Pilz et al. agree with other publications
- Holick 2024, 2025 (Endocr Pract): Both Pilz and Holick flag that retracting the 2011 guideline leaves populations (malabsorption, CKD, low measured 25(OH)D, established deficiency) without guidance. Pilz endorses Holick's suggestion to continue applying 2011 recommendations to those populations.
- Pludowski et al. 2024 (Nutrients): Pilz explicitly endorses 2,000 IU/day for adults as their expert-opinion default — directly aligning with Pludowski's review.
- Grant, Wimalawansa, Pludowski, Cheng 2025 (Nutrients) and Wimalawansa et al. 2024 (Nutrients): Shared view that Endocrine Society under-recognizes extra-skeletal benefits and that population-level recommendations need broader scope.
- Riedmann et al. 2025 / Alfredsson et al. 2020: Pilz frames sunlight/UV-B as the "elephant in the room" — agreeing with the growing literature that insufficient sun exposure is itself a public health problem and that UV confers non-vitamin-D-mediated benefits (mortality reductions in UK Biobank, Adventist Health Study 2).
- USPSTF / Choosing Wisely: Pilz accepts the broad anti-screening position but argues it's incomplete.
- Munns et al. 2016 (Global Consensus on Nutritional Rickets): Endorsed as the operative reference for infants <1 year.
Where Pilz et al. disagree or push back
- Against the Endocrine Society guideline itself — primary disagreements:
- 1. Dose vagueness. Stating "optimal doses are unknown" without providing a practical range is, per Pilz, an abdication. They explicitly endorse 2,000 IU/d as within the trial range for all four indications and safe.
- 2. No bridging for measured 25(OH)D. Real-world patients arrive with test results; the guideline gives no advice on interpreting them, including for values approaching the IOM 125 nmol/L "concern" threshold. Pilz proposes raising it to 150 nmol/L given 15+ years of new safety data (Billington 2020, Zittermann 2023, Cianferotti 2026, Malihi 2019).
3. Implementation void. The guideline implicitly recommends supplementation for ~50% of the US population but provides no implementation pathway.
Tension with Bolland 2021 / Breth-Petersen 2022: Those papers argue testing is wasteful; Pilz pushes for more nuanced guidance rather than blanket testing rejection.
Tension with newer evidence (which Pilz interprets generously toward the guideline):
- Jolliffe et al. 2025 (Lancet Diabetes Endocrinol) updated RTI meta-analysis lost overall statistical significance (OR 0.94, 95% CI 0.88–1.00); pediatric effect (1–15 y) preserved (OR 0.74, 0.60–0.92). Pilz judges this doesn't undermine the pediatric RTI recommendation but it weakens the all-ages story.
- Palacios et al. 2024 (Cochrane) pregnancy update removed 20 of 30 prior trials for trustworthiness concerns; significant outcomes contracted to severe postpartum hemorrhage and low birth weight. Pilz argues recommendations still hold; a stricter reader would say the evidence base has thinned.
- Thouvenot et al. 2025 (D-Lay MS, JAMA) — 100,000 IU q2wk in CIS reduced disease activity, also a safety signal at high intermittent doses, in some tension with the guideline's caution about ≥100,000 IU boluses.
Implicit disagreement with the more skeptical commentators (Pittas 2025 "In the Shadow of Enthusiasm"; the panel's own conservative posture): Pilz et al. are more pro-supplementation than the guideline authors. They cite Nwosu 2025 pediatric rebuttal but don't fully engage it.
Notable research gaps the authors flag
- No defined upper dose limit for empiric supplementation.
- No guidance for the ~10% (Switzerland data) to ~20% of populations who have been tested.
- Whether the IOM 125 nmol/L concern threshold should be revised upward.
- UV/sun exposure entirely absent from vitamin D guidelines globally.
- Implementation data — is the guideline actually changing practice?
The authors' AGREE II appraisal is in Supplementary Table S1 (not in the main text). Overall posture: methodologically rigorous guideline, but the conservative scope and silence on dose, testing, and replaced populations leave the practicing clinician without operational answers — a critique consistent with the broader European/Pludowski/Holick/Grant camp and at odds with the more minimalist US Endocrine Society/USPSTF position.
2024 Endocrine Society Guideline.pdf
Editorial of 5+ studies that disliked the 2024 guideline
Editorial: Impact of new vitamin D guidelines on pediatric and adult health: insights, evidence, and implications Editorial Front Endocrinol (Lausanne). 2026 Apr 29:17 doi: 10.3389/fendo.2026.1851754.
Clipped from 2-page PDF
"In a rebuttal to the 2024 Guideline (1), Nwosu rejects the sweeping one-size-fits-all recommendations, and the opaque recommendations for infants, children, adolescents, obese individuals,darkly pigmented individuals, pregnant women and fetuses. This rebuttal calls for routine screening, supplementation, and monitoring of serum 25(OH)D concentrations to ensure that everyone benefits from the skeletal and extra-skeletal actions of vitamin D."
"In conclusion, this Research Topic employed evidence-based and real-world research to examine the 2024 Endocrine Society Guideline on Vitamin D for Prevention of Disease by focusing on the role of vitamin D deficiency on childhood hypocalcemia; the health impact of disparate cut-off points for vitamin D status designation by different medical societies; the impact of high-dose vitamin D supplementation on T1D, T2D, and complete heart block; the negative impact of vitamin D deficiency in asthma, thyroid cancer, and diabetes mellitus. There is also the exciting possibility that transient overexpression of SDR42E1 gene can reverse these vitamin D deficiency states. These innovative works will spur further research in this field, and will shape future recommendations for vitamin D screening, monitoring, and supplementation."
A Continuing Medical Education compares 2011 and 2024
"Stop Testing Vitamin D in Healthy Patients, Says the Society That Told You to Start" (Medscape, July 23, 2026)
Medscape Table of Contents
Core premise
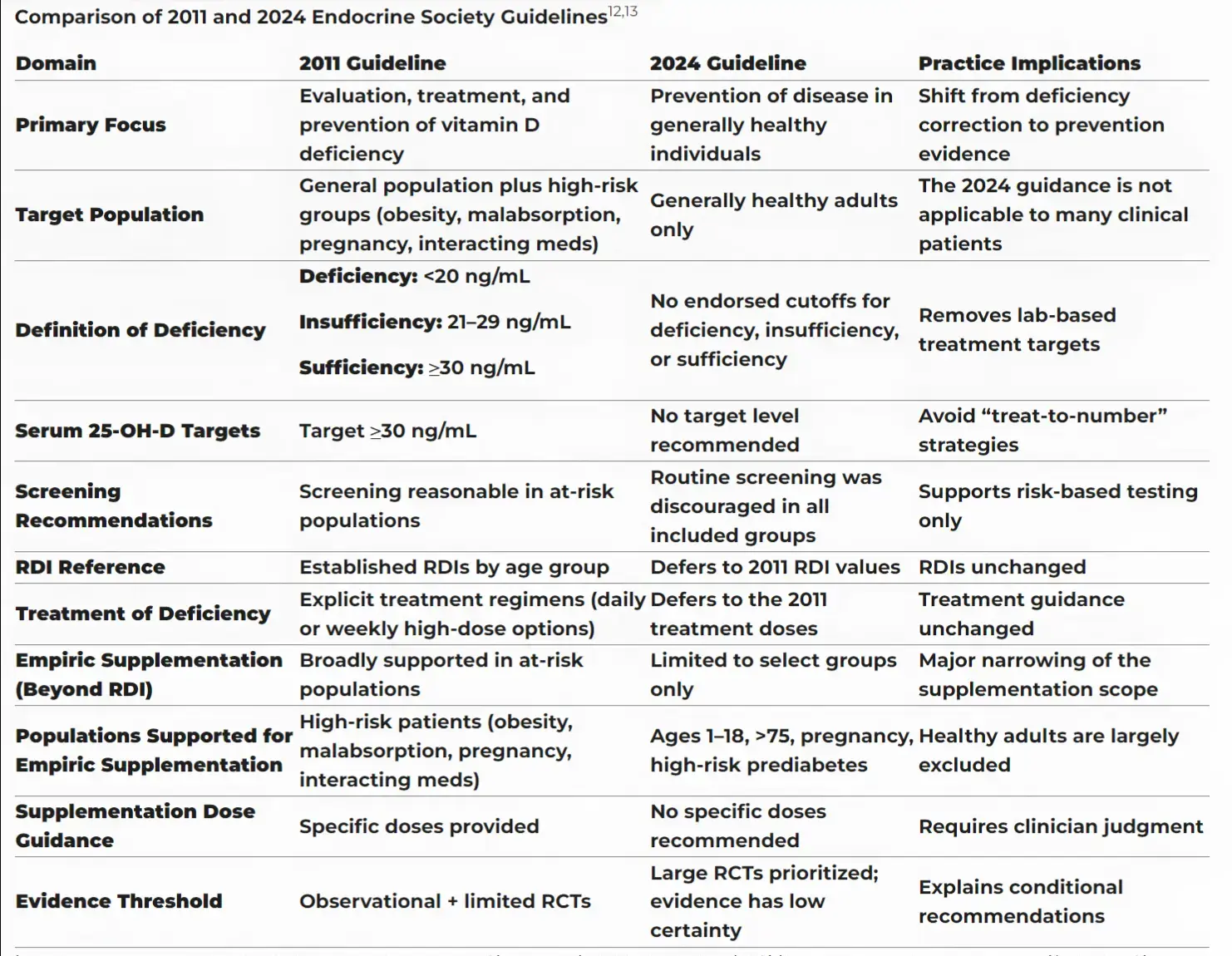
The article's hook is a practice-vs-guideline gap. The Endocrine Society abandoned its own 2011 30 ng/mL sufficiency threshold in the 2024 JCEM guideline and advised against routine 25(OH)D testing in healthy adults — but nobody updated the annual-physical order set. Vitamin D remains one of the most-ordered labs in US primary care and testing volume hasn't meaningfully changed since the reversal.
The 2024 guideline is actually narrower than 2011 in nearly every direction:
- Healthy adults under 75: suggests against supplementing beyond the RDA (600–800 IU/day), and against routine 25(OH)D testing.
- Explicitly includes obesity and darker skin pigmentation in the "don't test" category — both were flagged for testing in 2011.
- Declines to name any target blood level for disease prevention. Panel chair Marie Demay (Harvard/MGH) is quoted saying routine testing isn't recommended in any of the carve-out groups either.
The evidence base cited Four large, concordant null RCTs:
| Trial | Setting | Finding as characterized |
|---|---|---|
| VITAL | US, 25,871 adults | No reduction in cancer or CVD events |
| D-Health | Australia | Null |
| FIND | Finland | Null |
| DO-HEALTH | 5 European countries, 2000 IU/day, age 70+ | No benefit on fractures, infections, BP, physical performance, or cognition — despite 40% deficient at baseline |
The article presents DO-HEALTH as the answer to the "the null trials were all American" objection. USPSTF is noted as having called screening evidence insufficient twice (2014, 2021).
The two-camp framing
Presented as a rematch, not a new fight:
- IOM 2011: adequacy ≥20 ng/mL, covering 97.5% of the population; warned higher cut-points overstate deficiency prevalence.
- Endocrine Society 2011: ≥30 ng/mL, based on calcium-absorption and PTH-suppression data.
- 2024 ES guideline sides with IOM.
- Holick's rebuttal (Endocrine Practice, 2024) gets substantial space: the new document leaned too exclusively on RCTs and discounted association data on pregnancy outcomes, early childhood caries, autoimmune disease, URTIs including COVID-19, prediabetes progression, CVD, neurocognitive dysfunction, mortality, and cancer mortality.
Notably, the author concedes the dispute is unresolved: no trial has ever randomized patients to different serum targets, so both camps are weighting the same PTH and absorption data differently. The advice is to know which camp your specialist colleagues occupy before arguing over a 24 ng/mL result.
Four groups still get supplementation — without testing
- Children/adolescents (1–18): rickets prevention, possibly fewer respiratory infections
- Pregnancy: potential reduction in pre-eclampsia, preterm birth, neonatal mortality
- Adults 75+: modest mortality signal
- High-risk prediabetes: slower progression to diabetes
The article pressure-tests the prediabetes recommendation hardest: it rests on a pooled analysis of three trials showing 15% relative risk reduction (~3 percentage points absolute over 3 years, NNT ≈30) — but every constituent trial was null on its own primary endpoint, and one used an active vitamin D analogue rather than cholecalciferol. The ADA has seen the same data and declines to issue a positive recommendation. The article calls this "a live disagreement, not a rounding error."
Where testing still earns its keep
Unchanged from 2011 — CKD, malabsorption (celiac, IBD, bariatric surgery), granulomatous disease, hepatic failure, and enzyme-inducing medications. The point is emphasized: the guideline narrows testing in the general population, not in patients with actual impaired vitamin D metabolism.
The MS wildcard
D-Lay MS (JAMA 2025) is presented as the one recent countercurrent. Clinically isolated syndrome patients received 100,000 IU cholecalciferol every 2 weeks vs. placebo for 24 months:
- Disease activity (relapse or new MRI lesion): 60.3% vs 74.1%, HR 0.66 (95% CI 0.50–0.87), P=.004, NNT 7.2
- But driven by MRI lesion counts; clinical relapse alone was not significant (17.9% vs 21.8%, HR 0.69, 95% CI 0.42–1.16, P=.16)
- Single trial, narrow population (recent CIS, not established or progressive RRMS)
Conclusion drawn: a reason to check and correct vitamin D after a new demyelinating event; not evidence for population-wide bolus dosing.
Peer commentary quoted
- Manson: very limited role for both supplementation and screening in the general population
- F. Perry Wilson: describes vitamin D as, in his view, the molecule with the strongest correlation data and weakest causation data in all of clinical research
Practice bottom line
- 1. Don't screen asymptomatic healthy adults — evidence against benefit is now large, international, consistent.
- 2. For patients self-supplementing 1000–4000 IU/day: no trial evidence of harm at those doses; advising a return to RDA is reasonable but not mandatory, since the guideline addresses testing and new empiric prescribing, not existing supplementation.
- 3. Patients with obesity or darker skin already tested don't need retesting absent a new clinical indication.
- 4. Supplement without testing in the four carve-out groups (acknowledging ADA dissent on prediabetes).
- 5. Keep testing where a real disease process makes deficiency plausible.
- 6. First demyelinating event is the one place intermittent high-dose bolus now has trial support.
Observations
The piece is more concessive than its headline suggests — it explicitly grants that the 20 vs. 30 ng/mL question is unresolved by any trial, gives Holick's critique real space, flags the prediabetes recommendation as weakly supported, and states outright that there's no harm evidence at 1000–4000 IU/day. It also carries a linked deep-dive companion ("Vitamin D: A Low Number Is Not a Disease") and a ~50-item reference list, including a 2026 Clinical Nutrition mortality reanalysis (Wang/Brenner) and a 2026 APNM CVD meta-analysis that the article body doesn't actually discuss.
Related in VitaminDWiki
- US admits math mistake was made in 2010 in estimating Vitamin D, but will not change recommendations
- Consensus Vitamin D
- Vitamin D supplementation guidelines (adults – 50,000 IU per week)
- One pill every two weeks gives you all the vitamin D most adults need
- Vitamin D: 40-70 ng is optimal, sometimes more is needed - Grant, Sunil, Pawel, Cheng
- Comparing High-dose vitamin D therapies - may succeesful trials use cofactors and personalized dosing
- Vitamin D Cofactors in a nutshell
Other critiques of 2024 Endocrine Society