12 Strange Signs Your Body Needs Potassium - video
YouTube 13 minutes - 2025
Summary Glaspe and Claude AI
(00:01–02:45) Signs 1–5: Hand/finger cramps from disrupted electrical signals to muscles; post-meal tiredness from blood sugar swings; puffy eyes/facial swelling from kidneys retaining fluid; constipation due to weak smooth muscle contractions in the colon; and salty food cravings driven by cortisol depleting potassium.
(02:45–04:04) Signs 6–8: Muscle weakness and fatigue from low ATP production; hearing your pulse (swishing/throbbing in ears) from stiffened blood vessels, often after salty/sugary meals; and high blood pressure from narrowed arteries.
(04:04–06:05) Signs 9–11: Frequent nighttime urination from stored water/sugar being released overnight; fainting or dizziness (common on flights or after caffeine/alcohol) from poor blood and oxygen circulation; and mood swings/irritability from over-excited nerves.
(06:05–07:00) Sign 12 + bonus: Loud stomach growling from poorly contracting intestinal muscles; plus diabetes — diabetics are encouraged to aim for ~5,000 mg/day to reduce insulin resistance.
(07:00–07:27) Why testing fails: Only ~2% of body potassium is in blood, so standard blood tests routinely miss deficiencies.
(07:27–08:08) Why it matters: Potassium powers the sodium-potassium pump that lets cells generate energy; recommended intake is ~4,700 mg/day.
(08:08–09:27) Why deficiency is common: An estimated 98% of people in Western countries are deficient — driven by low vegetable intake, processed foods, high sodium, certain medications (diuretics, steroids, penicillin), stress, keto diets, vomiting/diarrhea, caffeine/alcohol, sweating, and low vitamin D.
(09:27–10:46) Food sources: Swiss chard, kale, avocado, beef liver, mushrooms, salmon, broccoli, pork tenderloin, Brazil nuts. A homemade electrolyte drink recipe is offered (avocado, lemon with peel, blueberries, Celtic sea salt, water).
(10:46–11:24) Lifestyle tweaks: Cut caffeine/alcohol/sugar/grains/processed foods; soak beans to reduce phytic acid; switch to Celtic sea salt; stay hydrated; supplement vitamin D3; use potassium-rich herbs (parsley, cilantro, basil, dill, oregano).
(12:06–12:47) Supplementation note: Capsules (~99 mg each) are impractical — would need ~47 pills daily. Half a teaspoon of potassium citrate powder in water adds ~1,000 mg. Balance with magnesium and sodium, and consult a doctor if you have kidney issues.
Note: This is a YouTube health video, not peer-reviewed guidance. Claims like "98% of people are deficient" and the 5,000 mg/day diabetes recommendation are stronger than mainstream evidence supports — the NIH/IOM Adequate Intake is 2,600–3,400 mg/day for adults, and upper-limit potassium supplementation can be genuinely dangerous for people with kidney disease or on certain medications (ACE inhibitors, ARBs, potassium-sparing diuretics).
Potassium association with Vitamin D
Answer first: No direct role
Potassium has no direct role in vitamin D synthesis or metabolism. It is not a cofactor for any of the vitamin D hydroxylases (unlike magnesium), and there is no credible evidence that potassium intake raises or lowers serum 25(OH)D. Every real association runs downstream of vitamin D's actions, converging on four pathways: urinary calcium/citrate handling and stone risk, the renin–angiotensin–aldosterone system (RAAS), blood pressure, and bone acid–base balance.
Two of these literatures actively undercut the simplest "they work together" story:
- The vitamin D → urinary-citrate mechanism is real in rats but null in humans.
- The "potassium protects bone" claim is, on the best randomized evidence, an alkali (bicarbonate/citrate anion) effect, not a potassium effect — potassium chloride does nothing.
The accurate framing: potassium's vitamin-D-relevant effects are largely calcium-oxalate-specific and anion-driven, and they matter for managing the consequences of vitamin D action (chiefly hypercalciuria and stones), not for vitamin D status itself.
Evidence by pathway
1. Urinary calcium, citrate, and kidney stones
Evidence tier: Strong (established therapeutic use + RCT) — but type-specific.
Potassium citrate is standard prophylaxis for calcium-oxalate stones. It raises urinary citrate above baseline and lowers urinary calcium, the latter through reduced intestinal calcium availability, reduced bone resorption, and increased renal tubular calcium reabsorption. Because vitamin D drives intestinal calcium absorption and can raise urinary calcium in susceptible people, potassium-citrate status modulates one of the main downside risks of aggressive D repletion. This is the one pathway where the two nutrients genuinely interact in clinical practice.
Two important qualifiers:
- Not protective for all stone types. In a hypercalciuria model, potassium citrate's accompanying rise in urine pH, oxalate, and phosphate increased calcium-phosphate (brushite/apatite) supersaturation. The benefit is specific to calcium-oxalate stones and can theoretically worsen calcium-phosphate disease.
- Vitamin D repletion in deficient stone-formers did not raise hypercalciuria risk. In an interventional study of vitamin-D-deficient stone formers, raising 25(OH)D from ~10 to ~44 ng/mL over 3 months significantly lowered PTH and increased urinary citrate (median 341 → 411 mg, P = 0.045), with no significant difference in the proportion developing a meaningful (≥15%) rise in urinary calcium. The authors concluded conventional-dose vitamin D in deficient patients may not increase hypercalciuria risk. The hypercalciuria signal appears mainly when vitamin D is paired with between-meal calcium supplementation.
2. Vitamin D → renal citrate metabolism
Evidence tier: Mechanistic/animal positive; human observational NULL.
In rats, vitamin D reduces mitochondrial citrate oxidation in renal cells, which raises urinary citrate excretion, and 1,25(OH)₂D₃ may modulate intracellular citrate transport. VDR gene polymorphisms may amplify these effects. However, when tested directly in humans, the Swiss Kidney Stone Cohort found no significant association between 1,25(OH)₂D₃ levels and urinary citrate excretion on multiple linear regression. The rodent mechanism should not be read as a human dose-response.
3. RAAS / aldosterone → potassium
Evidence tier: Mechanism well-grounded; human causal/effect-size evidence weak; serum-K endpoint not demonstrated.
Vitamin D is a negative endocrine regulator of the RAAS. Vitamin-D-deficient individuals show greater plasma angiotensin II, a trend toward higher plasma renin activity, and greater renal RAAS responsiveness, and there is a classic inverse correlation between 1,25(OH)₂D₃ and plasma renin activity. Mechanistically this provides an indirect bridge to potassium: deficiency → RAAS activation → higher aldosterone → renal potassium wasting.
Cautions: the human data are largely cross-sectional and cannot establish causality, and the interventional base is thin — a 2023 meta-analysis assessing vitamin D supplementation on PTH and RAAS markers pooled only five RCTs (~698 participants). The specific claim that vitamin D status meaningfully changes serum potassium is not cleanly demonstrated.
4. Bone / acid–base balance
Evidence tier: Good short-term RCT — but the effect belongs to the ANION, not potassium.
This is the headline correction. A double-blind trial (Dawson-Hughes et al., 2008, n = 171) randomized older adults to potassium bicarbonate, sodium bicarbonate, potassium chloride, or placebo, all on background calcium + vitamin D. Results:
- Bicarbonate (whether as the K or Na salt) lowered urinary calcium and the bone-resorption marker NTX (both P = 0.001).
- Potassium chloride did nothing — KCl vs placebo was null (P = 0.773), and the KCl-vs-KHCO₃ contrast was significant (P = 0.015).
- The active variable was net acid excretion (NAE), which tracked linearly with calcium and NTX excretion.
The authors explicitly attribute the benefit to reduced dietary acid load, not potassium. The widely cited association between high potassium intake and higher bone mineral density is most likely confounded: potassium-rich diets are fruit-and-vegetable-rich and therefore alkali-producing. A separate metabolic study (Maurer et al., 2003) reached the same conclusion — neutralizing the Western diet inhibits bone resorption independently of potassium intake. Longer (2-year) alkali trials are conflicting (one null, one favoring potassium citrate on bone loss), and all co-administered vitamin D, so none isolates a vitamin D × potassium interaction.
What this does NOT show
- No cofactor relationship. Potassium is not required for, and does not regulate, 25-hydroxylation or 1α-hydroxylation. Contrast magnesium, which is a genuine cofactor.
- No effect of potassium on vitamin D status. No credible evidence that dietary or supplemental potassium changes serum 25(OH)D.
- The citrate link does not transfer from rats to humans. Positive rodent mechanism, null human association.
- "Potassium for bone" is really "alkali for bone." Potassium chloride is inert in the best RCT; the bicarbonate/citrate anion carries the effect. Potassium is mostly a marker of an alkaline, produce-rich diet.
- Observational potassium–25(OH)D correlations are confounded by overall diet quality. High-potassium intake tags a whole-food dietary pattern; it is not evidence of a direct interaction.
- No RCT powered specifically on a vitamin D × potassium interaction for any endpoint (stones, BP, bone).
Bottom line for clinical/editorial use
Potassium matters to vitamin D users chiefly as potassium citrate for calcium-oxalate stone risk during aggressive repletion — and even there, conventional-dose D in deficient patients raises citrate and does not reliably provoke hypercalciuria. The bone and citrate "synergies" people expect either reassign to bicarbonate or fail to replicate in humans. This makes a more defensible and more interesting entry than a generic co-supplementation claim.
Key studies
| Study | Design | Pathway | Finding | Tier |
|---|---|---|---|---|
| Vitamin D supplementation in stone formers (Iran) | Interventional, deficient stone-formers, 3 mo | Stones/citrate | 25(OH)D 10→44 ng/mL; PTH down; urinary citrate up; no excess hypercalciuria | RCT-level |
| Swiss Kidney Stone Cohort (Clin Kidney J 2020) | Observational cohort | Citrate metabolism | No association of 1,25(OH)₂D₃ with urinary citrate in humans | Observational (null) |
| Krieger et al. (calcium-phosphate stone model) | Animal/mechanistic | Stones | K-citrate raises pH/oxalate/phosphate → ↑CaP supersaturation | Mechanistic |
| Forman/Li; Resnick (RAAS) | Human cross-sectional + animal | RAAS | Deficiency ↑ angiotensin II/renin; inverse 1,25D–PRA (r ≈ −0.65) | Mechanistic + observational |
| Khodadadiyan et al. 2023 | Meta-analysis, 5 RCTs (~698) | RAAS/PTH | Limited evidence base on supplementation effects | RCT (sparse) |
| Dawson-Hughes et al. 2008 | 4-arm double-blind RCT, n=171 | Bone/acid-base | Bicarbonate, not potassium, lowers urinary Ca and NTX; KCl null | RCT (anchor) |
| Maurer et al. 2003 | Human metabolic | Bone/acid-base | Diet neutralization inhibits resorption independent of K | Mechanistic/controlled |
References
- 1. Vitamin D supplementation and risk of hypercalciuria in stone formers. Urol J / PubMed 30851716.
- 2. Impact of potassium citrate on urinary risk profile … kidney stone formers in Switzerland. Clin Kidney J 2020;13(6):1037. (Swiss Kidney Stone Cohort)
- 3. Effect of potassium citrate on calcium phosphate stones in a model of hypercalciuria. PMC4657843.
- 4. Calcium and vitamin D supplementation and their association with kidney stone disease: a narrative review. Nutrients 2021;13(12):4363.
- 5. Forman JP et al.; Resnick LM et al. — vitamin D and the renin-angiotensin system. PMC3999581.
- 6. Khodadadiyan A et al. Vitamin D supplementation effects on 25(OH)D, 1,25(OH)₂D, PTH and RAAS: systematic review and meta-analysis. BMC Nutr 2023. PMC10652523.
- 7. Dawson-Hughes B et al. Treatment with potassium bicarbonate lowers calcium excretion and bone resorption in older men and women. J Clin Endocrinol Metab 2009;94(1):96–102. PMID 18940881 / PMC2630872.
- 8. Maurer M et al. Neutralization of Western diet inhibits bone resorption independently of K intake … Am J Physiol Renal Physiol 2003;284:F32–F40.
9. Dawson-Hughes B et al. Potassium bicarbonate supplementation lowers bone turnover and calcium excretion: a randomized dose-finding trial. J Bone Miner Res 2015. PMID 25990255.
Evidence tiers: RCT > observational/cohort > mechanistic/animal. Claims are graded individually; absence of a vitamin D × potassium interaction trial is noted where relevant.*
Related in VitaminDWiki
- Very rarely will Vitamin D cause Hypercalcemia – a simple diagnostic
- Hypercalcemia and Vitamin D - many studies
- High Sodium may not be the problem: used to get 16X more Potassium than Sodium
- Very low Potassium if diet does not have lots of fruits and vegetables
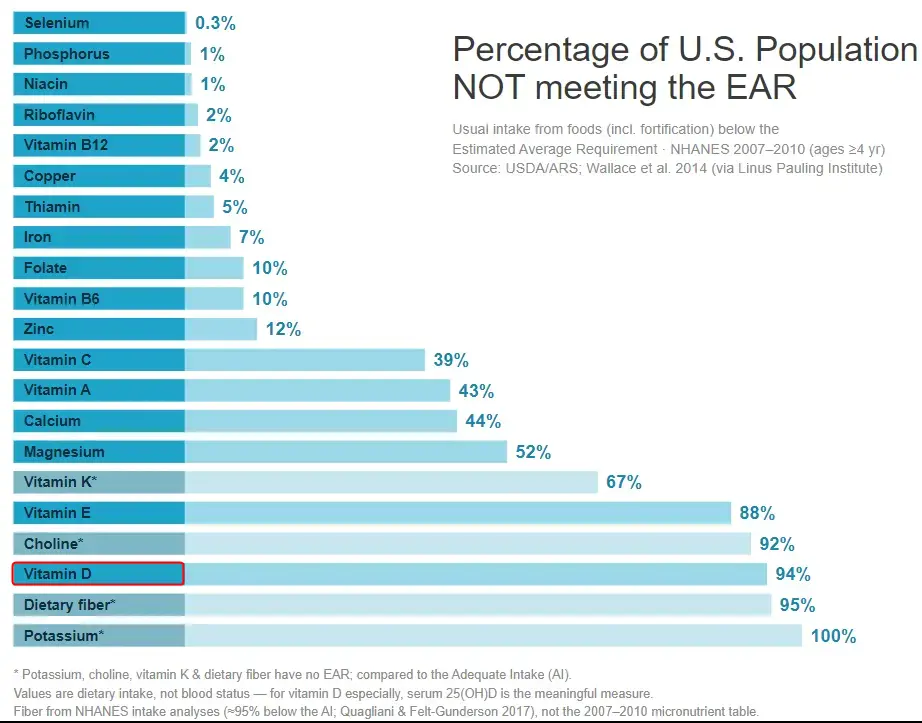
- People are not getting even the minimal nutrients, such as Vitamin D
100% are not getting Potassium EAR