High Sodium may not be the problem: used to get 16X more Potassium than Sodium
The Sodium-Potassium Paradox: Reexamining the Real Culprit in Cardiovascular Disease Perplexity AI - Jan 2026
Executive Summary
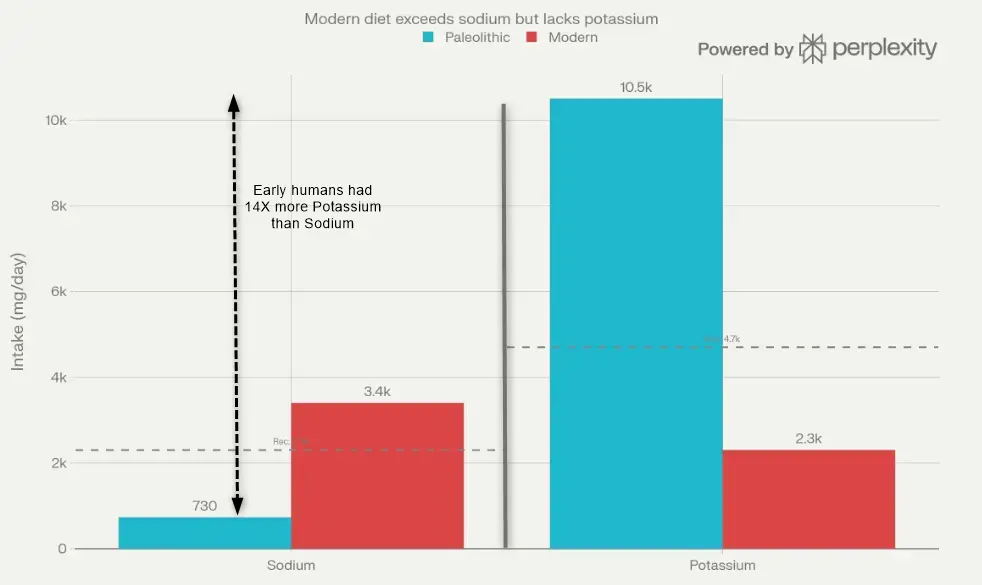
The evidence strongly indicates that inadequate potassium intake represents an equal or greater cardiovascular threat than excess sodium consumption. More precisely, the sodium-to-potassium ratio emerges as the most powerful dietary predictor of hypertension, stroke, and mortality—surpassing either mineral in isolation. Modern diets have created a profound evolutionary mismatch: humans evolved consuming roughly 10,500 mg of potassium and only 700 mg of sodium daily, yielding a protective 16:1 potassium-to-sodium ratio. Today's typical American diet has catastrophically inverted this pattern to approximately 1:1 or worse, with sodium intake increasing nearly fivefold while potassium intake has plummeted to less than one-fifth of ancestral levels. pmc.ncbi.nlm.nih
The Evolutionary Context: A 10,000-Year Mismatch
Ancestral Dietary Patterns
Analysis of Paleolithic diets reveals that pre-agricultural humans consumed approximately 690–768 mg of sodium per day (equivalent to 1.7 g of salt), primarily from naturally occurring sources in plants and animal tissues. Simultaneously, their plant-rich diets delivered an estimated 10,500 mg of potassium daily—more than four times current recommendations and nearly five times modern intake. This created a potassium-to-sodium ratio of approximately 16:1. pmc.ncbi.nlm.nih
Metabolic studies demonstrate that humans can maintain sodium balance at intakes as low as 100–375 mg per day, and contemporary hunter-gatherer societies such as the Yanomami Indians thrive on sodium intakes below 250 mg daily without signs of depletion or hypertension. These populations show virtually no age-related blood pressure increase, no cardiovascular disease, and normal physical activity in tropical climates—definitively proving that very low sodium intake supports optimal health when accompanied by adequate potassium. chriskresser
The Agricultural Revolution's Impact
The advent of agriculture approximately 10,000 years ago fundamentally altered human electrolyte consumption in two critical ways. First, the dietary foundation shifted from potassium-rich fruits, vegetables, tubers, and leafy greens to potassium-poor cereal grains (wheat, rice, maize). Second, the development of salt preservation technologies and the addition of sodium chloride to foods drove sodium consumption upward. pubmed.ncbi.nlm.nih
This timeframe represents merely 400–500 generations—insufficient for meaningful genetic adaptation. Human renal and cardiovascular physiology remains genetically "fixed in Paleolithic time," optimized for high potassium and low sodium intake. The resulting evolutionary mismatch between our Stone Age genome and modern electrolyte exposure underlies much of contemporary cardiovascular pathology. pubmed.ncbi.nlm.nih
Modern Dietary Reality
Current data from the National Health and Nutrition Examination Survey (NHANES) reveal that average American adults consume 3,400–3,746 mg of sodium daily—five times ancestral levels—while potassium intake has collapsed to 1,997–2,320 mg for women and 2,631–3,016 mg for men. This represents approximately 22% of ancestral potassium consumption. pmc.ncbi.nlm.nih
The statistics are sobering: more than 98% of Americans fail to meet minimum potassium recommendations, and fewer than 0.015% (roughly 1 in 6,600 people) simultaneously meet both sodium and potassium guidelines. This near-universal noncompliance suggests systemic food environment failure rather than individual dietary choice. nutritionfacts
Mechanistic Evidence: Why Potassium Deficiency Drives Hypertension
Renal Sodium Retention: The NCC Transporter System
Perhaps the most compelling mechanistic evidence emerges from research on the thiazide-sensitive sodium-chloride cotransporter (NCC) in the kidney's distal convoluted tubule. This transporter mediates 5–10% of total sodium reabsorption but plays an outsized role in blood pressure regulation and potassium homeostasis. pmc.ncbi.nlm.nih
Low extracellular potassium concentrations directly activate NCC through a voltage-dependent mechanism. Distal tubule cells detect potassium depletion via basolateral Kir4.1/Kir5.1 potassium channels, which causes membrane hyperpolarization and reduced intracellular chloride concentration. This releases inhibition of WNK (With No Lysine) kinases, which phosphorylate and activate NCC through the SPAK/OxSR1 kinase cascade. pmc.ncbi.nlm.nih
The result: enhanced sodium and chloride reabsorption, reduced sodium delivery to downstream potassium-secreting segments, volume expansion, and hypertension. Critically, this activation occurs independently of sodium intake. Conversely, high potassium intake dephosphorylates NCC within minutes, promoting natriuresis and potassium excretion. pubmed.ncbi.nlm.nih
Recent human studies in obese hypertensive adults confirmed that oral potassium produces rapid natriuresis approximately half the magnitude of hydrochlorothiazide (a thiazide diuretic that directly blocks NCC). This demonstrates the clinical relevance of potassium's NCC-regulatory effects in human hypertension. pubmed.ncbi.nlm.nih
Renin-Angiotensin-Aldosterone System (RAAS) Dysregulation
Low dietary potassium prevents normal suppression of the intrarenal renin-angiotensin system. In angiotensin II-dependent hypertensive animal models, potassium supplementation prevented the induction of angiotensinogen (AGT) expression in proximal tubules, collecting duct renin, and angiotensin-converting enzyme (ACE)—all components that contribute to intratubular angiotensin II formation and sodium retention. frontiersin
The synergistic effect of low potassium and high sodium creates a "perfect storm": high sodium should suppress RAAS activity through volume expansion and aldosterone feedback, but concurrent potassium deficiency prevents this normal homeostatic response. The result is inappropriate RAAS activation despite volume expansion—a state that perpetuates hypertension and end-organ damage. chriskresser
Vascular Pathophysiology
Beyond renal effects, potassium deficiency directly damages blood vessels through multiple pathways:
Vascular Calcification: Low potassium increases calcium levels within vascular smooth muscle cells, activating CREB (cAMP response element-binding protein) and promoting transformation of smooth muscle cells into bone-like cells—a process called vascular calcification. This contributes to arterial stiffness and atherosclerosis. High potassium supplementation reverses this process in animal models. stagetestdomain3.nih
Endothelial Dysfunction: Potassium deficiency impairs endothelial production of nitric oxide (NO) while increasing production of transforming growth factor-beta (TGF-β), a profibrotic molecule that promotes vascular stiffness. Dietary potassium inhibits salt-induced TGF-β production through activation of endothelial calcium-activated potassium (BK) channels. pmc.ncbi.nlm.nih
Inflammatory Activation: High sodium intake in the context of low potassium triggers interstitial sodium accumulation in tissues, leading to lymphangiogenesis mediated by macrophages and increased inflammatory responses. This inflammatory state contributes to salt-sensitive hypertension. pmc.ncbi.nlm.nih
Metabolic Acidosis: The Hidden Consequence
Modern diets rich in animal protein and sodium chloride but deficient in potassium-rich plant foods create chronic low-grade metabolic acidosis—a state of subtle but persistent acid-base imbalance. Potassium in fruits and vegetables exists primarily as alkaline salts (potassium citrate, potassium malate) that metabolize to bicarbonate, buffering dietary acid load. pubmed.ncbi.nlm.nih
This dietary acidosis has cascading effects: calcium mobilization from bone to buffer acids (contributing to osteoporosis), muscle protein catabolism, reduced growth hormone secretion, increased cortisol, and enhanced gluconeogenesis. Supplementation with potassium bicarbonate or potassium citrate reverses these effects without requiring sodium restriction, improving calcium balance, reducing bone resorption, enhancing nitrogen balance, and mitigating age-related decline in growth hormone. reddit
The Sodium-Potassium Ratio: A Superior Biomarker
Evidence from Observational Studies
Multiple large-scale prospective cohort studies demonstrate that the sodium-to-potassium ratio predicts cardiovascular outcomes more powerfully than either mineral alone. In a landmark analysis of 12,267 U.S. adults followed for 14.8 years, those in the highest quartile of sodium-potassium ratio (compared to the lowest) exhibited: contemporaryobgyn
- 46% higher risk of all-cause mortality (HR 1.46, 95% CI 1.18–1.81)
- 46% higher risk of cardiovascular mortality (HR 1.46, 95% CI 1.07–2.00)
- 115% higher risk of ischemic heart disease mortality (HR 2.15, 95% CI 1.48–3.12)
Importantly, these associations persisted across subgroups defined by sex, race/ethnicity, body mass index, hypertension status, education level, and physical activity—suggesting robust, generalizable effects. jamanetwork
Analysis of dose-response relationships reveals that per 1,000 mg/day increase in sodium, all-cause mortality risk rises 20% (HR 1.20), while per 1,000 mg/day increase in potassium, mortality risk falls 20% (HR 0.80). The multiplicative nature of these effects explains why the ratio captures risk more comprehensively than either component. jamanetwork
Potassium and Stroke Prevention
Meta-analyses consistently demonstrate a strong inverse relationship between potassium intake and stroke risk. Pooled analysis of 11 prospective studies encompassing 247,510 participants found that 1.64 g (42 mmol) per day higher potassium intake associated with a 21% lower risk of stroke (RR 0.79, 95% CI 0.68–0.90). An updated meta-analysis incorporating 14 cohorts (333,250 participants, 10,659 stroke events) confirmed this protective effect (RR 0.80, 95% CI 0.72–0.90). bjcardio.co
The magnitude of stroke risk reduction achieved through increased potassium intake rivals that expected from reducing sodium by 5 g (85 mmol) per day—translating to a potential prevention of 1.15 million stroke deaths annually worldwide. bjcardio.co
Blood Pressure Effects
Systematic reviews of randomized controlled trials demonstrate that increased potassium intake reduces blood pressure in both hypertensive and normotensive individuals. A 2013 Cochrane review of controlled trials found that increased potassium lowered systolic blood pressure by 3.49 mm Hg (95% CI 1.82–5.15) and diastolic pressure by 1.96 mm Hg (95% CI 0.86–3.06) in hypertensive adults. bmj
Dose-response analyses suggest maximal blood pressure reduction when potassium intake reaches 90–120 mmol/day (3,510–4,680 mg/day)—precisely the range recommended by the WHO and close to ancestral consumption patterns. The sodium-to-potassium ratio shows even stronger associations with blood pressure than absolute intakes, with optimal ratios approaching 1:1 or lower. econtent.hogrefe
Randomized Trial Evidence: Salt Substitutes Transform Outcomes
The Salt Substitute and Stroke Study (SSaSS)
The SSaSS trial represents the most definitive evidence to date that addressing potassium deficiency while reducing sodium yields profound cardiovascular benefits. This cluster-randomized trial conducted in 600 rural Chinese villages enrolled 20,995 participants with history of stroke or uncontrolled hypertension. pmc.ncbi.nlm.nih
Participants randomized to the intervention group received salt substitute (75% sodium chloride, 25% potassium chloride by mass) free of charge to replace all household salt use, while control villages continued using regular salt (100% sodium chloride). Over a mean follow-up of 4.7 years, the salt substitute group experienced: pmc.ncbi.nlm.nih
- 14% reduction in stroke (29.1 vs. 33.7 events per 1,000 person-years; HR 0.86, 95% CI 0.77–0.96; p=0.006)
- 13% reduction in major cardiovascular events (HR 0.87, 95% CI 0.80–0.94; p<0.001)
- 12% reduction in all-cause mortality (39.3 vs. 44.6 deaths per 1,000 person-years; HR 0.88, 95% CI 0.82–0.95; p<0.001)
Critically, rates of serious hyperkalemia did not differ between groups, refuting concerns that potassium-enriched salt substitutes pose safety risks in populations with normal kidney function. Post-hoc analyses confirmed benefits were consistent across age, sex, baseline blood pressure, and medication use. pmc.ncbi.nlm.nih
Meta-Analysis of Salt Substitute Trials
A comprehensive meta-analysis incorporating 23 randomized controlled trials (32,073 participants, follow-up 4 weeks to 10 years) evaluated salt substitutes—typically replacing 25–50% of sodium chloride with potassium chloride. Compared to regular salt, participants consuming salt substitutes achieved: pmc.ncbi.nlm.nih
- Systolic blood pressure reduction of 4.80 mm Hg (95% CI −6.12 to −3.48; p<0.0001)
- Diastolic blood pressure reduction of 1.48 mm Hg (95% CI −2.06 to −0.90; p<0.0001)
- 12% reduction in all-cause mortality (HR 0.88, 95% CI 0.82–0.94; p=0.0003)
- 28% trend toward reduced cardiovascular mortality (HR 0.72, 95% CI 0.52–1.00; p=0.05)
These benefits emerged alongside significant reductions in 24-hour urinary sodium excretion (−22.96 mmol/24-h) and increases in potassium excretion (+14.41 mmol/24-h), confirming adherence and biological effects. pmc.ncbi.nlm.nih
The POTCAST Trial: High-Normal Potassium Targets
In 2025, the POTCAST trial provided novel evidence that targeting high-normal potassium levels (4.5–5.0 mmol/L) reduces arrhythmia burden and cardiovascular events in high-risk patients. This open-label randomized trial enrolled 1,200 participants with implantable cardioverter-defibrillators (ICDs) and baseline plasma potassium ≤4.3 mmol/L. escardio
Participants randomized to the intervention received dietary counseling, potassium supplements, and/or mineralocorticoid receptor antagonist (MRA) therapy to raise plasma potassium to 4.5–5.0 mmol/L. After a median 39.6-month follow-up, the high-normal potassium group achieved mean potassium levels of 4.36 mmol/L versus 4.05 mmol/L in controls. escardio
The primary composite endpoint (sustained ventricular tachycardia, appropriate ICD therapy, hospitalization for arrhythmia/heart failure, or death) occurred in 22.7% of the high-potassium group versus 29.2% of controls—a 24% relative risk reduction (HR 0.76, 95% CI 0.61–0.95; p=0.015). Appropriate ICD therapies decreased 25%, and hospitalizations for cardiac arrhythmias fell 37%, with no increase in hyperkalemia-related adverse events. escardio
These findings suggest that even modest increases in potassium levels within the normal range confer cardiovascular protection—a paradigm shift challenging conventional fear of potassium supplementation.
The Role of Ultra-Processed Foods
Modern ultra-processed foods (UPFs) systematically worsen the sodium-potassium imbalance. In the United States, more than 75% of dietary sodium derives from sodium added during food processing and manufacturing, with only 10–12% from naturally occurring sources and table salt. The top 10 food categories—bread, cold cuts, pizza, poultry, soups, sandwiches, cheese, pasta dishes, meat dishes, and savory snacks—contribute 44% of total sodium intake. stacks.cdc
Conversely, food processing removes or dilutes naturally occurring potassium. Analysis of NHANES data demonstrates an inverse dose-response relationship between the percentage of calories from ultra-processed foods and dietary content of potassium, fiber, magnesium, and vitamins. As UPF consumption increases from the lowest to highest quintile, potassium density falls significantly, while sodium, saturated fat, and added sugars rise. pmc.ncbi.nlm.nih
The dietary sodium-to-potassium ratio increases dramatically with higher UPF consumption. Those reporting frequent use of industrialized condiments exhibited significantly higher urinary sodium-to-potassium ratios, confirming that processed food consumption is the primary driver of the modern electrolyte mismatch. pubmed.ncbi.nlm.nih
Importantly, potassium exists in whole foods as organic salts (potassium citrate, potassium malate) that provide alkaline buffering capacity, whereas potassium chloride added to processed foods lacks this benefit. This distinction underscores the superiority of obtaining potassium from fruits, vegetables, legumes, and unprocessed foods rather than supplements or fortification alone. stacks.cdc
Limitations of Sodium-Only Approaches
Conflicting Evidence and Methodological Issues
Several observational studies, most notably the Prospective Urban Rural Epidemiology (PURE) study, reported J-shaped or U-shaped relationships between sodium intake and cardiovascular outcomes, suggesting harm at both very low and very high intakes. These findings generated controversy and challenged recommendations for population-wide sodium reduction below 2,300 mg/day. phri
However, the PURE study has been extensively critiqued for methodological flaws. It estimated 24-hour sodium excretion from single fasting morning spot urine samples using the Kawasaki equation—a method shown to have large systematic and random error. This approach "markedly alters the association of sodium to blood pressure relative to measured 24-hour urine sodium". In 2023, the World Hypertension League, International Society of Hypertension, and Resolve to Save Lives issued a joint policy statement declaring: "It is strongly recommended to not conduct, fund, or publish research studies that use spot urine samples with estimating equations to assess individuals' sodium (salt) intake in association with health outcomes". pmc.ncbi.nlm.nih
Meta-analyses of randomized controlled trials using gold-standard 24-hour urine collections consistently demonstrate linear, graded associations between sodium reduction and blood pressure lowering at intakes exceeding 800 mg/day, with no evidence of J-curves. The apparent harm at very low sodium intakes in observational studies likely reflects reverse causation (sick individuals restricting sodium), confounding, or measurement error rather than true biological effects. bmj
Sodium Restriction in Heart Failure: The Potassium Connection
Recent evidence suggests that sodium restriction without attention to potassium may fail to improve—or even worsen—outcomes in patients with chronic heart failure. A 2023 meta-analysis found that sodium restriction in heart failure patients was associated with a higher risk of the composite endpoint of mortality and hospitalizations (OR 4.12, 95% CI 1.23–13.82) and did not significantly affect all-cause mortality or heart failure hospitalizations individually. pmc.ncbi.nlm.nih
This paradox may reflect several mechanisms. First, aggressive sodium restriction activates the renin-angiotensin-aldosterone system and sympathetic nervous system as compensatory responses to perceived volume depletion. Second, many heart failure patients take medications (ACE inhibitors, angiotensin receptor blockers, aldosterone antagonists) that impair potassium excretion, and stringent dietary restrictions may simultaneously limit potassium intake from natural food sources. my.clevelandclinic
Third—and most importantly—sodium restriction interventions in these trials occurred in isolation, without concomitant potassium optimization. By contrast, salt substitute interventions that reduce sodium while increasing potassium consistently show cardiovascular benefits. This suggests that the sodium-potassium balance, rather than sodium reduction alone, determines clinical outcomes. pmc.ncbi.nlm.nih
Clinical and Public Health Implications
Recommended Targets and Food Sources
Current guidelines recommend potassium intakes of at least 3,510 mg/day (WHO) to 4,700 mg/day (U.S. Dietary Guidelines for Americans), with sodium restricted to less than 2,000–2,300 mg/day. However, as demonstrated earlier, fewer than 2% of Americans meet potassium targets, and virtually none achieve both goals simultaneously. bmjopen.bmj
The optimal strategy emphasizes increasing consumption of potassium-rich whole foods rather than relying primarily on sodium restriction. The richest sources include: stacks.cdc
- Vegetables: spinach, Swiss chard, beet greens, potatoes, sweet potatoes, tomatoes, Brussels sprouts (200–900 mg per serving)
- Fruits: bananas, oranges, cantaloupe, honeydew, apricots, dried fruits (250–500 mg per serving)
- Legumes: white beans, lentils, kidney beans, soybeans (400–800 mg per serving)
- Dairy: milk, yogurt (300–400 mg per serving)
- Fish: salmon, halibut, tuna (400–500 mg per serving)
- Nuts and seeds: almonds, pistachios, sunflower seeds (200–300 mg per ounce)
Achieving ancestral potassium intakes of 10,500 mg/day would require consuming approximately 8–10 servings of fruits and vegetables daily—a target that, while aspirational, aligns with diets associated with exceptional longevity and freedom from chronic disease (Mediterranean, DASH, traditional Japanese diets). pubmed.ncbi.nlm.nih
Salt Substitutes: A Pragmatic Population Strategy
Given the difficulty of achieving dietary change at the population level, potassium-enriched salt substitutes represent a highly pragmatic intervention. These products—typically containing 65–75% sodium chloride and 25–35% potassium chloride—can be substituted 1:1 for regular salt in cooking and food manufacturing with minimal taste differences at appropriate replacement levels. pmc.ncbi.nlm.nih
Economic modeling suggests widespread adoption of salt substitutes in key food categories (bread, processed meats, cheese, soups, sauces) could substantially increase population potassium intake while reducing sodium, bringing average intakes closer to WHO recommendations without requiring dramatic dietary overhaul. The FDA has issued guidance recognizing potassium chloride as a valuable sodium replacer and permitting its declaration on food labels. pmc.ncbi.nlm.nih
Safety concerns about hyperkalemia appear largely unfounded in populations with normal kidney function. The SSaSS trial, POTCAST trial, and meta-analyses found no increased risk of hyperkalemia-related adverse events with potassium supplementation or salt substitutes. Caution remains warranted in patients with advanced chronic kidney disease (eGFR <30 mL/min/1.73m²), those taking potassium-retaining medications, or individuals with known hyperkalemia, but these represent a minority of the population. my.clevelandclinic
Reframing Public Health Messaging: "Add potassium, reduce sodium" or "Fix the ratio."
Current public health campaigns overwhelmingly emphasize sodium reduction through messages such as "cut the salt" or "sodium kills." While not incorrect, this framing ignores the equally—if not more—important role of potassium insufficiency. Messaging should evolve to emphasize the sodium-potassium balance: "Add potassium, reduce sodium" or "Fix the ratio."
This reframing aligns with positive dietary guidance that encourages consumption of nutrient-dense whole foods rather than solely restricting processed foods. It also acknowledges the evolutionary mismatch underlying modern cardiovascular disease and provides a coherent explanation for why plant-rich dietary patterns consistently associate with superior health outcomes. pubmed.ncbi.nlm.nih
Limitations and Future Research Directions
Despite the compelling evidence assembled here, several limitations warrant acknowledgment. First, most mechanistic studies linking potassium deficiency to NCC activation, RAAS dysregulation, and vascular dysfunction derive from animal models. While human studies of sodium-potassium balance and blood pressure support these mechanisms, direct demonstration of these pathways in humans remains incomplete. pmc.ncbi.nlm.nih
Second, long-term randomized controlled trials of potassium supplementation (without concurrent sodium reduction via salt substitutes) are limited. Most evidence for potassium's cardiovascular benefits comes from observational cohorts with residual confounding potential. Ongoing trials such as the dietary counseling and potassium supplementation studies in chronic kidney disease populations will provide valuable additional data. bmj
Third, the optimal sodium-potassium ratio for cardiovascular health remains uncertain. While ancestral ratios approached 1:16 and current recommendations implicitly target ratios near 1:2 (2,300 mg sodium, 4,700 mg potassium), it is unclear whether achieving these ancestral extremes would provide additional benefits beyond intermediate targets. Dose-response analyses suggest diminishing returns at very high potassium intakes, though the upper threshold remains undefined. bmjopen.bmj
Fourth, the role of other dietary factors—particularly the source and form of potassium (organic salts versus potassium chloride), calcium, magnesium, and overall dietary acid-base balance—deserves further investigation. Evidence suggests potassium from whole foods provides superior benefits compared to potassium chloride supplements, possibly due to accompanying nutrients, fiber, and buffering capacity. stacks.cdc
Finally, longer follow-up of the SSaSS cohort will be valuable for evaluating effects on cancer outcomes, chronic kidney disease progression, and other endpoints beyond cardiovascular disease. Adjudication of all events (not just fatal outcomes) and extension of follow-up duration would enhance statistical power and capture delayed effects of long-term electrolyte modification. pmc.ncbi.nlm.nih
Conclusion
The preponderance of evidence indicates that the modern epidemic of hypertension and cardiovascular disease reflects a profound evolutionary mismatch between our Paleolithic genome and contemporary electrolyte intake patterns. While excessive sodium consumption receives deserved attention, inadequate potassium intake represents an equal or greater threat, and the sodium-to-potassium ratio emerges as the most powerful dietary determinant of cardiovascular outcomes.
Multiple lines of evidence converge on this conclusion:
Evolutionary: Humans evolved consuming 10,500 mg potassium and 700 mg sodium daily (16:1 ratio); modern diets have catastrophically inverted this pattern to 2,300 mg potassium and 3,400 mg sodium (1:1.5 ratio). pmc.ncbi.nlm.nih
Mechanistic: Potassium deficiency activates renal sodium retention via NCC, prevents normal RAAS suppression, promotes vascular calcification and stiffness, impairs endothelial function, and creates metabolic acidosis—all independent pathways to hypertension and cardiovascular disease. pubmed.ncbi.nlm.nih
Observational: The sodium-potassium ratio predicts all-cause mortality, cardiovascular mortality, and stroke more powerfully than either mineral alone, with high ratios increasing mortality risk by 46–115%. econtent.hogrefe
Interventional: Salt substitutes (reduced sodium + added potassium) reduce stroke by 14%, major cardiovascular events by 13%, and all-cause mortality by 12% in randomized trials, while potassium-only supplementation reduces stroke risk by 21–24%. bmj
The question posed—"Is high sodium the problem or is the real problem much lower potassium?"—presents a false dichotomy. Both factors matter, but their ratio determines cardiovascular risk more precisely than either alone.
In practical terms, this means effective prevention strategies must simultaneously reduce sodium intake (primarily by limiting ultra-processed foods) and increase potassium consumption (primarily by increasing whole plant foods). Salt substitutes offer a pragmatic, scalable approach to achieving both goals.
Public health policy should evolve from exclusive focus on sodium reduction toward dual emphasis on optimizing the sodium-potassium balance. Given that 98% of Americans fail to meet potassium recommendations while 98% exceed sodium recommendations, and that addressing both through dietary modification or salt substitutes yields dramatic cardiovascular benefits, this reframing could transform cardiovascular disease prevention. bmjopen.bmj
After thousands of years eating a high-potassium, low-sodium diet, our species now confronts the metabolic consequences of a radical—and recent—dietary transformation. The remedy lies not in pharmaceutical intervention alone, but in realigning our food environment with our evolutionary biology: more potassium, less sodium, and restoration of the protective ratio that sustained human health for millennia.
Short answer: it’s probably both—but the potassium drop is the bigger, quieter shift we tend to ignore.
Longer answer, with some evolutionary context 👇
Chat-GPT Jan 2026
1. Sodium didn’t suddenly explode — potassium collapsed
If you look at estimates of pre-agricultural / pre-industrial diets:
- Potassium: ~7,000–10,000 mg/day
- Sodium: ~500–1,000 mg/day
- Na:K ratio: ~1:10 or better
Modern Western diets flip this on its head:
- Potassium: ~2,000–2,800 mg/day (often less)
- Sodium: ~3,000–4,000+ mg/day
- Na:K ratio: ~2:1 or worse
So yes, sodium went up—but potassium fell off a cliff.
That ratio change is probably the most physiologically important part.
2. Potassium is the primary counter-regulator to sodium
Potassium isn’t just “another electrolyte”:
- Drives natriuresis (kidneys excrete sodium when potassium is adequate)
- Relaxes vascular smooth muscle → lower blood pressure
- Improves endothelial function
- Dampens renin-angiotensin-aldosterone system (RAAS) overactivation
- Stabilizes cardiac electrical activity
When potassium intake is low:
- Sodium sensitivity increases
- Blood pressure rises at lower sodium levels
- Vascular stiffness increases
- Stroke risk rises independent of sodium intake
This is why in many populations, high sodium only predicts hypertension when potassium is low.
3. Evidence from populations & trials
Some key observations:
Hunter-gatherer and rural agrarian societies
- Very high potassium
- Often moderate sodium
- Near-zero hypertension across lifespan
INTERSALT & PURE studies
- Sodium alone ≠ consistent predictor of mortality
- Low potassium strongly predicts cardiovascular risk
- Best outcomes occur with high potassium + moderate sodium
DASH diet
- Blood pressure reduction tracks more with potassium, magnesium, and food matrix than sodium restriction alone
Salt restriction trials
- Effects are highly variable
- Sodium-sensitive individuals benefit
- Others show minimal or adverse hormonal responses (↑ renin, ↑ aldosterone)
4. Why sodium got blamed historically
A few reasons sodium became the villain:
- Easy to isolate and reduce
- Clear short-term BP response in salt-sensitive people
- Potassium is harder to supplement safely in trials
- Food industry sodium → processed foods → guilt by association
- Early hypertension models ignored evolutionary context
But sodium restriction without potassium repletion can worsen:
- Insulin resistance
- Sympathetic activation
- Fatigue and dizziness
- Arrhythmia risk in vulnerable people
5. More accurate to say: The sodium–potassium balance is profoundly abnormal
It’s not:
“Sodium is high”
It’s:
“The sodium–potassium balance is profoundly abnormal.”
From a physiological standpoint:
- Humans evolved in a high-potassium environment
- Our kidneys, vasculature, and nervous system still assume that context
- Modern diets violate that assumption daily
6. Practical takeaway (non-medical)
For most people without kidney disease or potassium-handling disorders:
- Prioritize potassium-rich whole foods (leafy greens, legumes, tubers, squash, avocado, fruit)
- Moderate, not eliminate, sodium
Avoid the trap of:
“Low sodium + low potassium + ultra-processed food”
That combo is likely the worst of all worlds.
Bottom line: High sodium is a stressor. Low potassium removes the buffering system. The real problem is the loss of the buffer.
Related in VitaminDWiki
- Early humans had much higher levels of: Vitamin D, Vitamin C, Iron, Zinc, Potassium, etc
- Very low Potassium if diet does not have lots of fruits and vegetables
- Potassium helps bones by increasing the absorption of both Calcium and Vitamin D
- Off topic: Low salt is actually bad for you - IoM reversal Summer 2013
- Off topic – myth that should have low salt diet
Sodium Potassium ratio: 4 million items in Google Scholar
- Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase - 2017 PDF