Overview Hyperparathyroidism and vitamin D
Know Your D: book authored in June 2010 by Dr. Keebler,
got me to look up the topic on the web Sept 2010
pg 150 Be careful adding large amounts of vitamin D to the elderly.
The incidence of primary hyperparathyroidism increases steadily with age.
At age 60. 2 in 1000 women and 1 in 1,000 men have it
By age 90, 60 in 1000 women and 30 in 1,000 men - many undiagnosed
pg 138 Dr, Keebler describes the reactions of giving extra vitamin D to a 77-year-old man who had undiagnosed hyperparathyroidism
In a few weeks: became thirstier than usual, complained of feeling confused and tired, and had little appetite, and extra pains
Vitamin D level was only 27 ng/ml, but Calcium level was 12 mg/ml - whereas normal is about 10 ng/ml
Appears that should have a blood test for vitamin D AND Calcium seniors
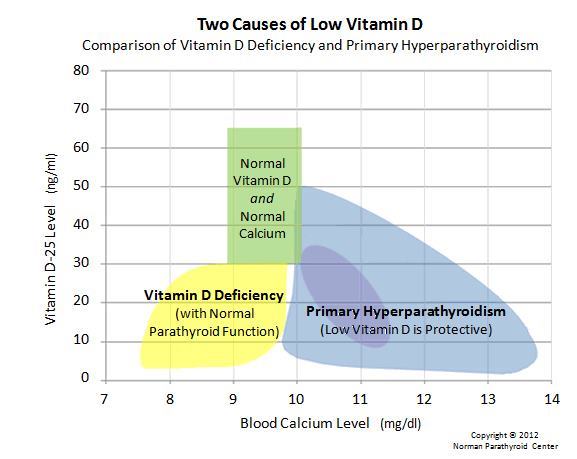
Good Overview at Parathyroid.com - updated March 2013, has the following graphic
Yet Another Reason to Take Vitamin D WEB MD April 2000
Vitamin D Deficiency and Secondary Hyperparathyroidism in the Elderly: Consequences for Bone Loss and Fractures and Therapeutic Implications
Endocrine Reviews 22 (4): 477-501; Copyright © 2001 by The Endocrine Society; Paul Lips p.lips@vumc.nl
Department of Endocrinology, Institute for Endocrinology, Reproduction, and Metabolism (EVM-Institute) and Institute for Research in Extramural Medicine (EMGO-Institute), Vrije Universiteit Medical Center, 1007 MB Amsterdam, The Netherlands
Vitamin D deficiency is common in the elderly, especially in housebound and in geriatric patients. Establishing strict diagnostic criteria is hampered by differences in assay methods for 25-hydroxyvitamin D. The synthesis of vitamin D3 in the skin under the influence of UV light decreases with aging due to insufficient sunlight exposure and a decreased functional capacity of the skin. The diet contains a minor part of the vitamin D requirement. Vitamin D deficiency in the elderly is less common in the United States than elsewhere due to the fortification of milk and the use of supplements. Deficiency in vitamin D causes secondary hyperparathyroidism, high bone turnover, bone loss, mineralization defects, and hip and other fractures. Less certain consequences include myopathy and fall. A diet low in calcium may cause an increased turnover of vitamin D metabolites and thereby aggravate vitamin D deficiency. Prevention is feasible through UV light exposure, food fortification, and supplements. Vitamin D3 supplementation causes a decrease in serum PTH concentration, a decrease in bone turnover, and an increase in bone mineral density. Vitamin D3 and calcium may decrease the incidence of hip and other peripheral fractures in nursing home residents. Vitamin D3 is recommended in housebound elderly and may be cost-effective in hip fracture prevention in selected risk groups.
Hyperparathyroidism and How It's Related to Vitamin D which follows
Hyperparathyroidism and how it's related to Vitamin D have always been a subject of discussion among medical experts. There are two types of hyperparathyroidism: primary and secondary. Primary hyperparathyroidism is defined as a disorder in the parathyroid glands which means that there is too much secretion of parathyroid hormone (PTH) from one or more overactive, enlarged parathyroid glands. Secondary hyperparathyroidism is a disorder, such as kidney failure, that causes the over-activity o parathyroids. Vitamin D is needed for strong bones - quite unrelated to hyperparathyroidism. This is the main reason why hyperparathyroidism and how it's related to Vitamin D is often discussed.
If there is too much secretion of hormones from parathyroid glands, which is the main condition of primary hyperparathyroidism, there is a disruption in the balance, causing the blood calcium to rise. The condition of too much calcium in the blood is called hypercalcemia, which doctors usually use to suspect disorder in the parathyroid glands. The excessive PTH triggers the over-secretion of calcium into the! Bloodstream. Because of this, the bones may lose a large amount of calcium but may increase in the urine, causing kidney disorders called kidney stones . PTH can also lower the levels of blood phosphorus by increasing the phosphorus excretion in the urine. A person diagnosed with hyperparathyroidism may experience subtle symptoms, severe ones, or none at all.
Calcium and Vitamin D supplements are known as the primary treatments for hyperparathyroidism regardless of the cause, with the only difference that arises from the parathyroid hormone's inactivity due to hypomagnesemia. Since parathyroid hormone or PTH is necessary for kidneys to produce an active form of Vitamin D, patients diagnosed with hyperparathyroidism do not have enough PTH; thus, these patients cannot naturally produce enough Vitamin D needed to absorb calcium in the intestines. Thus, it is easy to understand hyperparathyroidism and its relation to Vitamin D because the two are intertwined. While its cause is unknown, doctors and medical experts use Vitamin D to treat this disease, at least as a supplemental treatment. Patients diagnosed with hyperparathyroidism are advised to take supplemental Vitamin D orally.
Primary hyperparathyroidism in a vicious cycle with vitamin D – safe to add - Nov 2011
Primary hyperparathyroidism - Is vitamin D supplementation safe?
Aust Fam Physician. 2011 Nov;40(11):881-4.
Rankin W. BAppSc, BMBS, Ph.D., MAACB, is a basic physician trainee,
Division of Medicine, Flinders Medical Centre, Bedford Park, South Australia.
Background Vitamin D deficiency is commonly seen in patients with primary hyperparathyroidism.
However, there is a widespread reluctance to supplement this group of patients with vitamin D.
Objective This article examines the relationship between vitamin D deficiency and primary hyperparathyroidism and the effects of vitamin D supplementation.
Conclusion Vitamin D deficiency exacerbates primary hyperparathyroidism and vice versa .
With care, vitamin D supplementation can safely be given to selected patients with asymptomatic primary hyperparathyroidism and is suggested before deciding on medical or surgical management.
Monitoring serum calcium concentration and urinary calcium excretion is recommended while achieving vitamin D repletion.
PDF is attached at the bottom of this page
Secondary Hyperparathyroidism reduced with paricalcitol – Nov 2011
Effectiveness of treatment with oral paricalcitol in patients with pre-dialysis chronic kidney disease.
Nefrologia. 2011 Nov 25;31(6):697-706. doi: 10.3265/Nefrologia.pre2011.Aug.11030.
[Article in English, Spanish]
Hervás Sánchez JG, Prados Garrido MD, Polo Moyano A, Cerezo Morales S.
Purpose: Secondary hyperparathyroidism is a common complication in patients with chronic kidney disease. Treatment with paricalcitol, a selective vitamin D receptor (VDR) activator, has shown benefits in these patients by adequately reducing PTH levels with minimal changes in serum calcium and phosphorus.
The aim of this study was to assess the effectiveness and safety of paricalcitol in chronic renal disease patients (CKD grades 3 and 4). Methods: A study of our experience with paricalcitol was conducted in normal clinical practice in patients over 18 years diagnosed with grade 3 or 4 chronic kidney disease. Patients were periodically evaluated every 3 months. The primary endpoint of effectiveness was to obtain two consecutive decreases of (greater than or equal to) 30% in iPTH with respect to baseline values. The secondary endpoints were the fulfillment of the objectives in accordance with the Spanish Society of Nephrology (SEN) and Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines, as well as the relationship between the effectiveness of the treatment and different patient variables. Safety was studied by means of hypercalcemia events.
Results: The primary study endpoint was achieved in 54.3% of patients. In addition, another 16.3% of patients had reduced iPTH by more than 30% at the 3rd visit. Therefore, 70.6% of patients reduced their iPTH levels by more than 30% in 6 months. The relationship between treatment success, glomerular filtration rate, and body mass index was significant. There were few adverse events, although hypercalcemia was found in 5.4% of patients.
Conclusions: Paricalcitol treatment effectively controls secondary hyperparathyroidism in non-dialyzed patients with a wide safety margin.
PMID: 22130286
WikiPedia Paricalcitol clips
Paricalcitol (marketed by Abbott Laboratories under the trade name Zemplar ) is a drug used to prevent and treat secondary hyperparathyroidism (excessive secretion of parathyroid hormone) associated with chronic renal failure. Chemically, it is 19-nor-1,25-(OH)2-vitamin D2 or 19-nor-1,25-dihydroxyvitamin D2, being an analog of 1,25- Dihydroxyergocalciferol, the active form of vitamin D2.
Side effects
Paricalcitol has been evaluated for safety in clinical studies in 454 chronic renal failure stage 5 patients. In four placebo-controlled, double-blind, multicenter studies, discontinuation of therapy due to any adverse event occurred in 6.5% of 62 patients treated with paricalcitol and 2.0% of 51 patients treated with placebo for 1 to 3 months.
Potential adverse events of paricalcitol injection are, in general, similar to those encountered with excessive vitamin D intake. Signs and symptoms of vitamin D intoxication associated with hypercalcemia include:
Early: Weakness, headache, somnolence, nausea, vomiting, dry mouth, constipation, muscle pain, bone pain, and metallic taste.
Late: Anorexia, weight loss, conjunctivitis (calcific), pancreatitis, photophobia, rhinorrhea, pruritus, hyperthermia, decreased libido, elevated blood urea nitrogen, hypercholesterolemia, elevated AST and ALT, ectopic calcification, hypertension, cardiac arrhythmias, somnolence, death, and rarely, overt psychosis.[4]|
WikiPedia Secondary hyperparathyroidism introduction
Secondary hyperparathyroidism refers to the excessive secretion of parathyroid hormone (PTH) by the parathyroid glands in response to hypocalcemia (low blood calcium levels) and associated hypertrophy of the glands. This disorder is especially seen in patients with chronic renal failure.
WikiPedia Primary hyperparathyroidism introduction
Primary hyperparathyroidism causes hypercalcemia (elevated blood calcium levels) through the excessive secretion of parathyroid hormone (PTH), usually by an adenoma (benign tumor) of the parathyroid glands.
The prevalence of primary hyperparathyroidism has been estimated to be 3 in 1000 in the general population and as high as 21 in 1000 in postmenopausal women.[3]
It is almost exactly three times as common in women as in men.
PMID: 22059217
See also VitaminDWiki
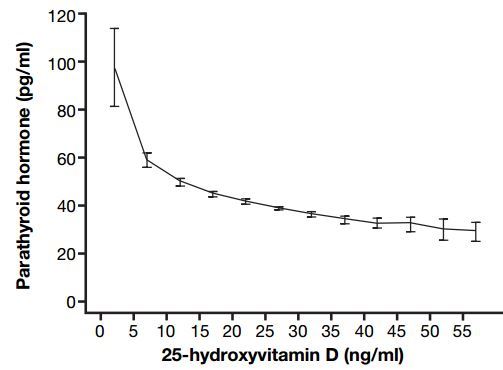
Need 40 ng of vitamin D to have proper PTH levels – May 2011
Parathyroid – Vitamin D inflection points might be at both 16 and 32 ng – Oct 2019
Patent to treat secondary hyperparathyroidism with 30 ng Vitamin D – March 2018
Hypothyroidism risk reduced 32 percent in those getting vitamin D levels above 50 ng – Oct 2017
Parathyroid Hormone levels increase 63 percent with age (33,000 people) – Sept 2017
Hypothesis Vitamin D receptor controls PTH without needing Vitamin D – Aug 2015
2800 IU of vitamin D before and after parathyroid surgery helped a lot – RCT Jan 2014
Hypothesis: Primary hyperparathyroidism might increase when vitamin D levels increase – Aug 2012
PTH does not plateau with increasing vitamin D, but does decrease with patient age – Aug 2012
Search VitaminDWiki for hyperparathyroidism 853 items as of July 2016
Primary Hyperparathyroidism perfectly predicted with a Vitamin D-Based nomogram – Nov 2011
50,000 IU vitamin D weekly is safe and effective for Primary Hyperparathyroidism – Jan 2013
Graves Disease is 2.2X more likely with low vitamin D – meta-analysis May 2015
See also web
Rockwell announced launching Calcitriol injection for secondary hyperparathyroidism in May 2012
A New, Vitamin D-Based, Multidimensional Nomogram for the Diagnosis of Primary Hyperparathyroidism July 2012
StopThe Thyroid Madness is a great website and book available in English, German, and Swedish
- discusses vitamin D, rebels against standard TSH tests, focuses on body temperature
- Hyperparathyroidism - Analysis and Market Forecasts to 2019 70 page report $6000, Nov 2012
- table of contents is free; Theglobal hyperparathyroidism therapeutics market is forecast to grow to reach $2.6 billion by 2019.
- Vitamin D supplementation in primary hyperparathyroidism, not a bad idea? Vitamin D Council, July 2013
- Vitamin D Council discussion is behind a $5/month paywall
- Discussion is based on Prolonged treatment with vitamin D in postmenopausal women with primary hyperparathyroidism. Full free text online
- Primary hyperparathyroidism and metabolic risk factors, impact of parathyroidectomy and vitamin D supplementation, and results of a randomized double-blind study Oct 2013
- Clinical Trial using 1600 IU of vitamin D: was not enough