Oral calcidiol is a good form of vitamin D supplementation
Clin Cases Miner Bone Metab. 2017 May-Aug;14(2):207-208. doi: 10.11138/ccmbm/2017.14.1.207. Epub 2017 Oct 25.
Piergianni Biondi Jessica Pepe Federica Biamonte Marco Occhiuto Martina Parisi Chiara Demofonti Valeria Baffa Salvatore Minisola Cristiana Cipriani cristiana.cipriani@gmail.com
Department of Internal Medicine and Medical Disciplines, “Sapienza” University of Rome, Rome, Italy
📄 Download the PDF from VitaminDWiki
Summary
Vitamin D supplementation represents an important topic in the field of metabolic bone disease. Calcidiol, the 25-hydroxy-vitamin D [25(OH)D], is the form of vitamin D most recently introduced in clinical practice. Advantages of the use of calcidiol derive from the pharmacokinetic properties and are related to the possibility of use in patients with liver disease, obese patients, patients with intestinal malabsorption, secondary hyperparathyroidism associated with chronic kidney disease as well as to avoid any possible toxic effect when high doses are used. The ADDI-D study demonstrated the efficacy and safety of calcidiol at the daily dose of 20 or 40 μg and 125 μg/week. In particular, the daily dose of 40 μg can be suggested as an alternative in severely deficient patients, as it has demonstrated to ensure higher vitamin D levels, compared to the 20 μg/day and the weekly 125 μg dose. The last can be an option when issues with compliance to the supplementation are present..
Vitamin D deficiency is a very common condition in the elderly and in young adults, with many clinical consequences, mostly in relation to the role of the hormone in the regulation of skeletal and calcium metabolism and in many other systems. The classical actions of vitamin D include regulation of mineral homeostasis of the skeleton by promoting calcium and phosphorus absorption in the gut to ensure adequate serum concentrations and mineralization of bone. Among non-classical target tissues, the parathyroid glands, the neuromuscular and immune system, heart, vessels, cancer cells, and gastrointestinal tissues have been studied (1, 2). The association between vitamin D deficiency and increased risk of many chronic conditions has been extensively described in observational studies investigating the effect of the hormone on the aforementioned “classical” and “non-classical” target organs (2, 3). Available evidence indicates that 25(OH)D serum levels > 30 ng/mL (75 ni cl'-) are desirable in all subjects, particularly patients at high risk for falls and fracture, and before the initiation of b one-active drugs (4). Conversely, intervention studies on the extra-skeletal effects of vitamin D supplementation showed so far inconsistent results.
In general, the issue of vitamin D supplementation is one of the most important in the clinical management of deficient states, particularly as far as form, doses and dose schedule to be used. The two main forms of vitamin D employed for suppler ani, tion -..e cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2). In particular, oral cholecalciferol demonstrated in many studies to be superior to ergocalciferol in rapidly and safely increase vitamin D serum levels in deficient and insufficient patients (5, 6). Both the pro-hormones are biologically inactive and hydroxylated in the liver to 25- hydroxy-vitamin D [25(OH)D], or calcidiol. The second hy- droxylation occurs primarily in the kidney to form the physiologically active 1,25-dihydroxy-vitamin D [1,25(OH)2D], or calcitriol. As far as recommendation on dose regimes, a daily administration of 1,500-2000 IU of cholecalciferol is warranted in adult deficient patients (4). Also, the use of loading doses, followed by a daily or monthly regimen after the threshold for sufficiency is reached, is recommended for severely deficient patients (4, 7).
Among other precursors of vitamin D employed in clinical practice, calcidiol is the most recently introduced for treatment of hypovitaminosis D (8). Pharmacokinetic studies demonstrated the hydrophilic properties of calcidiol, as well as a shorter half-life (10-13 days) in comparison with cholecalciferol (9). These data suggest the possible advantage of calcidiol, compared to cholecalciferol, in the management of deficient states in patients with liver disease, obese patients (where there is a lower trapping of calcidiol vs cholecalciferol in the adipose tissue), as well as to avoid any possible toxic effect when high doses are used (10). Also, conditions associated with intestinal malabsorption can represent an indication for calcidiol use, as it is better absorbed than cholecal- ciferol. The use of calcidiol in the setting of secondary hyperparathyroidism associated with chronic kidney disease has also been advocated, as high PTH levels can inhibit the liver cytochrome and eventually reduce the synthesis of calcidiol (11). Finally, data on the immunological effect of calcidiol vs cholecalciferol suggest a possible use in patients at high risk of infections (12).
As far as dose regimen, studies have shown that daily, weekly or monthly administrations of calcidiol are safe and effective in increasing and maintaining optimal 25(OHD) serum levels (8, 13). Corresponding doses are as follows: daily 15-20 microg, weekly 105-140 microg, and monthly 500 microg. The daily dose of 20 microg and the monthly dose of 140 microg demonstrated to be more effective and rapid than the corresponding cholecalciferol doses in enhancing serum 25(OH)D levels in healthy postmenopausal women (13). Similar results were observed for the 140 microg bolus (13). As far as clinical outcomes, calcidiol showed beneficial effect on muscle performance, lower extremity function and blood pressure (14). There are few data on the long-term skeletal effects of calcidiol and few studies have compared different therapeutic regimens in terms of effect on vitamin D status and bone metabolism.
The ADDI-D (Administration of Different Doses of calcidiol) study is a multicenter, randomized, open label study designed at evaluating the effects of three different regimens of oral calcidiol in post-menopausal women aged 55 and older with baseline serum 25(OH)D levels < 30 ng/mL (15). A total of 87 women were randomized to 3 different dose regimens, as follows: calcidiol 20 microg/day (27 subjects); calcidiol 40 microg/day (28 subjects); calcidiol 125 microg/week (29 subjects) (15). Follow-up time was 90 days, with monitoring visits performed once a week for the first month and at 60 days. All regimens resulted in a significant increase in serum levels of 25(OH)D at the end of the treatment period. The average serum levels of 25(OH)D were similar at any time point in the group placed on 20 microg/day and the one on 125 microg/week, while patients on 40 microg/day had almost doubled levels (15). Adequate vitamin D levels [25(OH)D concentration > 30 ng/mL] were observed in all subjects after 14 days, with a further increase thereafter, and a plateau between 30 and 90 days. Concomitantly, there was a significant increase of serum vitamin D binding protein levels up to 4 weeks. No safety issue (hypercalcemia, hypercalciuria) was registered in the observation period and serum 25(OH)D maintained in the range 30-100 ng/ml. Bone markers, 1,25(OH)2D and FGF-23 remained within the normal range for the duration of the study with no statistical difference between the groups, while PTH levels significantly decreased equally in the 3 groups at 90 days. Results from the ADDI-D study further clarify the role of calcidiol in improving vitamin D status and define alternative regimens to be used in clinical practice. In particular, the daily dose of 40 microg can be suggested as an alternative in severely deficient patients, as it has demonstrated to ensure higher vitamin D levels, while the weekly 125 microg dose can be an opt. ” when issues with compliance to the supplementation are present.
In conclusion, calcidiol has demonstrated to be effective in rapidly and safely improve vitamin D status and maintain adequate vitamin D serum levels with positive effect on the vitamin D target organs. To this end, different dose regimens have been suggested by the studies, showing that the daily 20 microg or 40 microg can be good options, while the weekly 125 microg and the monthly 500 microg may be used to improve compliance. More data from randomized controlled trials are needed in order to clarify the skeletal effect of calcidiol, particularly on fracture risk, as well as the effect on non-skeletal tissues.
References
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-81.
Minisola S, et al. A reappraisal of vitamin D effect on nci-skeletal targets and mortality. J Endocrinol Invest. 2015;38(11):1239-41.
Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008;87(4):1080S-6S.
Holick MF, et al. Evaluation, treatment, ar 1 p'.vention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):19.1- .0.
Cipriani C, et al. Long-term bioavailability after a single oral or intramuscular administrate ■ of 600,. 00 IU of ergocalciferol or cholecalciferol: implications for treatment and prophylaxis. J Clin Endocrinol Metab. 2013;98(7):2709-15.
Romagnoli E, et al. Short and long-term variations in serum calciotropic hormones after a single very large dose of ergocalciferol (vitamin D2) or cholecalciferol (vitamin D3) in the elderly. J Clin Endocrinol Metab. 2008;93(8):3015-20.
Rossini M, et al. Guidelines for the diagnosis, prevention and management o. 'steoporosis. Reumatismo. 2016;68(1):1-39.
Russo S, et al. Metabolic changes following 500 mug monthly administration of calcidiol: a study in normal females. Calcif Tissue Int. 2011;89(3):252-7.
Brandi ML, Minisola S. Calcidiol [25(OH)D3]: from diagnostic marker to therapeutical agent. Curr Med Res Opin. 2013;29(11):1565-72.
Cianferotti L, et al. The clinical use of vitamin D metabolites and their potential developments: a position statement from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the International Osteoporosis Foundation (IOF). Endocrine. 2015;50(1):12-26.
Michaud J, et al. Reduced hepatic synthesis of calcidiol in uremia. J Am Soc Nephrol. 2010;21(9):1488-97.
Bischoff-Ferrari HA, et al. Oral supplementation with 25(OH)D3 versus vitamin D3: effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J Bone Miner Res. 2012;27(1):160-9.
Jetter A, et al. Pharmacokinetics of oral vitamin D3 and calcifediol. Bone. 2013.
Meyer O, et al. Calcifediol versus vitamin D3 effects on gait speed and trunk sway in young postmenopausal women: a double-blind randomized controlled trial. Osteoporos Int. 2015;26(1):373-81.
Minisola S, Biondi P, Pepe J, Cipriani C, Fossi C, Giusti F, Franceschelli F, Leoncini Gz, Brandi ML. Calcifediol: perspectives for clinical applications in 2017 - control of mineral metabolism: the ADDID study. 2017.
Related in VitaminDWiki
- Is HyD (25(OH)D) a better form of vitamin D for some animals and maybe humans with liver problems
- Calcidiol may be 5X more effective than Vitamin D3 – June 2012
- Calcifediol (Calcidiol) might be a better form of Vitamin D for some people – May 2019
- Calcidiol category
- Google Scholar: 251 studies referenced this study as of Dec 2025
- Cholecalciferol or Calcifediol in the Management of Vitamin D Deficiency May 2020 FREE PDF
- Hypovitaminosis D: Is It Time to Consider the Use of Calcifediol? May 2019 FREE PDF
- Effects of Weekly Supplementation of Cholecalciferol and Calcifediol Among the Oldest-Old People: Findings From a Randomized Pragmatic Clinical Trial Nov 2019 FREE PDF
- Getting Vitamin D into your blood and cells has the following chart
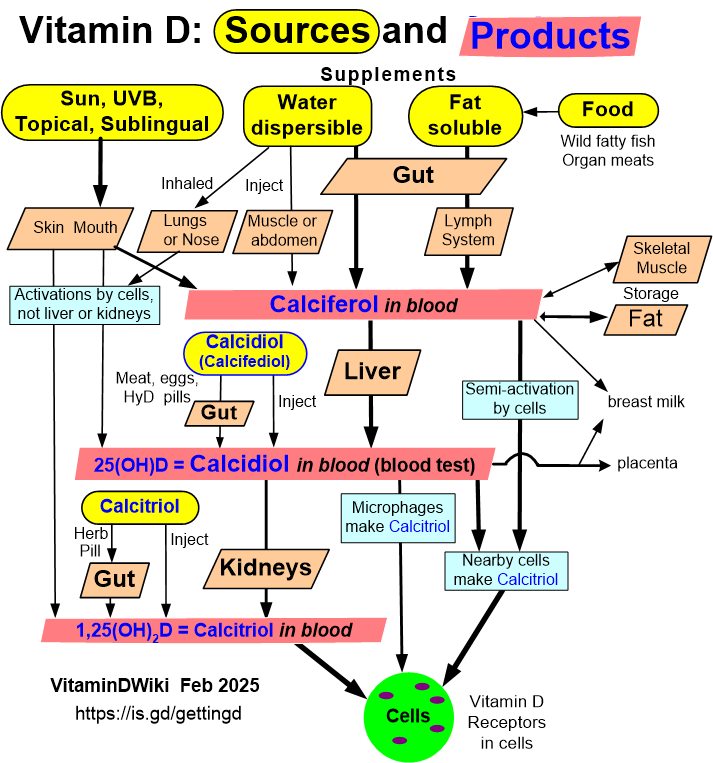
The gut does not need to digest fat in order to digest Calcidiol
Also, Calcidiol does not need the lymph system nor the liver