Dry Eyes treated by Omega-3 and Vitamin D – many studies
12+ VitaminDWiki pages have DRY EYE in the title
This list is automatically updated
{LIST()}
Dry Eye Disease associated with increase of 4 diseases (all associated with low vitamin D) - Oct 2024
PDF abstract contains
Adjusted for medical comorbidities (i.e., hypothyroidism, Sjögren's syndrome, systemic lupus erythematosus), participants with DED had higher odds than controls in having a
depressive disorder (odds ratio (OR): 3.47; 95% CI: 3.32-3.62),
anxiety (OR: 2.74; 95% CI: 2.63-2.85),
bipolar disorder (OR: 2.23; 95% CI: 2.04-2.44), and
schizophrenia spectrum disorder (OR: 2.48; 95% CI: 2.17-2.84).
The association between DED and mental health conditions was stronger in
Black participants than White participants (OR: 3.68 vs. 3.09, P<0.001).
Note: Blacks often have much lower vitamin D levels than whites
Can Vitamin D Help with Dry Eyes? - July 2025
Canadian Opthomological Society
review of the study: Safety and Efficacy of Topical Vitamin D in the Management of Dry Eye Disease Associated With Meibomian Gland Dysfunction: A Placebo-Controlled Double-Blind Randomized Controlled Trial - May 2024 10.1097/ICO.0000000000003400 PDF is behind paywall used topical vitamin D drops for 8 weeks
People with Dry Eye Disease have 3.99 ng/mL lower levels of Vitamin D - Oct 2024
Details with hyperlinks at Perplexity AI
VitaminDWiki - Sjögren’s syndrome (2nd most common rheumatic disease) and vitamin D - many studies
"Sjögren's syndrome is a chronic autoimmune disorder where the immune system mistakenly attacks and damages the body's moisture-producing glands."
People with Dry Eye Disease had 7X less expression of Vitamin D Receptor (not seen by Vitamin D test) - May 2024
Low Expression of Vitamin D Receptor in Patients With Dry Eye Disease
Cornea. 2024 May 14. doi: [10.1097/ICO.0000000000003555] PDF behind paywall
Antonia Vieira 1, Javiera Meza 2, Rodolfo Garreton 1, Arturo E Grau 1, Pablo Zoroquiain 2
Purpose: This study aimed to compare the expression of vitamin D receptor (VDR) on the ocular surface of patients with dry eye disease (DED) and controls without ophthalmological pathologies.
Methods: Patients with DED without previous treatment were studied and compared with healthy subjects. Ocular Surface Disease Index assessement and ocular surface cytology were performed in all patients. The immunohistochemical expression of VDR was evaluated using fully automated immunohistochemistry. The evaluation involved multiplying the percentage of nuclear-labeled cells (0-100) by their intensity (0-3), resulting in a score ranging from 0 to 300 (VDR H-score). Squamous metaplasia was morphologically evaluated using liquid-phase cytology with Papanicolaou/periodic acid-Schiff staining using Nelson's grade (scale 0-3, higher grade to higher metaplastic change).
Results: Eighteen patients with DED without previous treatment and 10 healthy subjects were studied. Squamous metaplasia was observed in 74% of patients with DED, in contrast to 0% in the control group. In patients with DED, there was a lower expression of VDR than in the control group (VDR H-score: 11.2 ± 13.9 vs. 80.9 ± 56; P = 0.0001). Furthermore, an inverse correlation was observed between Nelson grade and VDR H-score (P = 0.0001, rs = -0.71). No correlation was observed between Ocular Surface Disease Index and VDR H-score.
Conclusions: This is the first study to evaluate the VDR in patients with DED. These patients presented with a lower expression of VDR than healthy subjects. No correlation was found with more severe symptoms. Patients with DED also had a higher frequency of squamous metaplasia.
Eye doctor cured his own Dry Eyes by taking Omega-3 for 60+ days - May 2023
I Took Omega 3 Fish Oil for 90 days, Here's What Happened - YouTube - DoctorEyeHealth
Started with an Omega-3 index test = 4.3
Daily measured his "dry eyeness" with his eye testing machines

Ended with an Omega-3 index test = 9.5 and virtually no dry eyes
Previous video on The Omega-3 he took
He has many previous dry-eye videos - that did not apparently help
Note: his diet was plant-based, so contained little Omega-6, which could have blocked Omega-3
Dry Eye Disease: What Is the Role of Vitamin D? - Jan 2023
Int. J. Mol. Sci. 2023, 24(2), 1458; https://doi.org/10.3390/ijms24021458
by Maurizio Rolando 1ORCID andStefano Barabino 2,*ORCID
1 Ocular Surface and Dry Eye Center, Is.Pre Oftalmica, 16129 Genoa, Italy
2 Ocular Surface and Dry Eye Center, ASST Fatebenefratelli-Sacco, Ospedale Sacco-Università di Milano, 20157 Milan, Italy
Note: Studies have not yet tried topical vitamin D, does not mention Omega-3 and Dry Eyes
Dry eye disease (DED) is a multifactorial condition resulting from reduced tear secretion from the lacrimal glands, increased tear water evaporation or the production of poor-quality tears. Such tear instability can lead to inflammation and damage of the ocular surface, as well as to abnormal nociception. Historically, tear substitutes and corticosteroids have been the bastion of DED therapy, but a substantial number of patients still suffer from residual symptoms even after being treated with traditional treatments. Aiming to find safe and effective alternative therapies, recent efforts have been focused on the role of vitamin D in the cellular physiology of the eye. Possibly because of its positive effect in modulating the immune and inflammatory responses, the systemic supplementation of vitamin D seems, indeed, to be an effective therapeutic strategy, especially, but not only, for patients affected by DED that does not respond to conventional treatments. In this context, this review focuses on the literature reporting on the pathogenesis and treatment of DED, with a special emphasis on the recent investigations reporting on the potential role of the systemic administration of vitamin D as a therapeutic approach in the management of such condition.
📄 Download the PDF from VitaminDWiki
Omega-3 helps Dry Eye - Meta-analysis April 2019
Effects of Polyunsaturated Fatty Acids on Nonspecific Typical Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials
Nutrients 2019, 11(5), 942; https://doi.org/10.3390/nu11050942
Sheng-Chu Chi 1,2OrcID, Hsin-I Tuan 3,4OrcID and Yi-No Kang 5,*OrcID
To investigate the effects of polyunsaturated fatty acids (PUFAs) in patients with dry eye disease (DED), a multifactorial inflammatory disorder, we searched Cochrane Library, EMBASE, PubMed, and Web of Science for randomized clinical trials (RCTs) investigating the effect of PUFAs in patients with DED before March 2019. Two reviewers independently abstracted data of tear breakup time (TBUT), Schirmer’s test, osmolarity, and ocular surface disease index (OSDI). We conducted pairwise meta-analysis using means and standard deviations (SDs) in a random-effects model for continuous outcomes. Thirteen eligible RCTs with 1782 patients with nonspecific typical DED were included.
Patients who received PUFA treatment without other eye medications exhibited greater improvements in
TBUT (MD = 1.80; p = 0.001),
Schirmer test scores (MD = 0.50; p < 0.001),
osmolarity (MD = −15.95; p < 0.001), and
OSDI scores (MD = −10.19; p < 0.001)
than those who received placebo treatment.
However, the effects of PUFAs on TBUT (p < 0.001) and OSDI scores (p = 0.03) weakened with treatment duration. PUFAs are effective in treating nonspecific typical DED, particularly as a short-term treatment, with relatively few adverse events. Therefore, in real-world clinical practice, PUFA supplements are worth being suggested to patients with nonspecific typical DED who are not concurrently using other topical or systematic eye medications
📄 Download the PDF from VitaminDWiki
The Role of Omega-3 Essential Fatty Acids in Dry Eye Disease - Dec 2017
International Journal of Clinical and Experimental Ophthalmology 2017; 1: 055-059.
William J Faulkner, Cincinnati Eye Institute, 1945 CEI Dr, Blue Ash, OH 45242, USA, Wfaulkner@cincinnatieye.com
📄 Download the PDF from VitaminDWiki
One of every four visits to eye care professionals is for dry eye disease which affects an estimated 7-34% of Americans [1]. Knowledge regarding etiology and treatments has advanced exponentially in the last 20 years. As recently as 1997, in the mega textbook Cornea, it was stated “The mechanism for lacrimal gland dysfunction in this condition is unclear” [2]. A recent study entitled “The Dry Eye Workshop ll Report”, defines dry eye as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film and accompanied by ocular symptoms in which tear film instability and hyperosmolarity, ocular surface inflammation, and damage and neurosensory abnormalities play etiological roles” [3]. A 2003 study regarding the morbidity ratings of dry eye showed utility assessments for moderate and severe dry eye were parallel to historical reports for more severe (class lll/ lV) angina [4]. The tear film is responsible for the greatest optical power of any ocular surface, since the greatest change in the index of refraction occurs between the air and the tear film [5]. Double pass retinal imaging shows increased light scatter in dry eye patients which can decrease retinal image quality 20-40% [5]. Ophthalmologists now understand the critical necessity to normalize the ocular surface prior to cataract surgery; otherwise, they risk an unhappy patient with a less than ideal visual result. Increased use of electronic devices, such as smart phones, tablets, and computers, by youth in the last ten years has resulted in a broader age range of dry eye patients, to now include adolescents and teens.
A study of urban school age children showed that 8.2% had dry eye ( vs 2.8% in a rural group ), presumably due to high incidence of smart phone use.6 In fact, with cessation of phone use for four weeks, dry eye resolved completely in 100% of subjects [6]. Only two FDA approved dry eye medications are available: cyclosporine ophthalmic emulsion, 0.05%, (approved in 2003) and lifitegrast, 5%, (approved in 2016), both of which require chronic treatment. The focus of this discussion involves an emerging paradigm in treating ocular surface disease: a nutraceutical containing omega-3 essential fatty acids.
Dry eye disease may be broadly characterized as aqueous deficient (quantity) or evaporative (quality). In one large study, 86% of patients with dry eye disease had an evaporative component due to meibomian gland disease, (MGD) [7]. The Meibomian glands secrete meibum, the oil stabilizing the tear film, essential for a normal tear break up time and a moist cornea. MGD is characterized by terminal duct obstruction and/or qualitative/ quantitative changes in glandular secretion. Clinical signs include foam formation at the lid margin due to break down of lipids from soaps to free fatty acids (saponification), a toothpaste-like secretion upon attempted gland expression- also seen by meibomography, and a rapid tear break up time (TBUT).
Dietary patterns present for hundreds or thousands of years have changed in recent times. Essential fatty acids, only available through ingested food, fall into two major groups, Omega-3 and Omega-6 fatty acids, and are a requirement for multiple biological processes in the body. The ideal ratio in the body of Omega-3/6 is 1/1 but with contemporary diets rich in animal fats, vegetable oils and processed foods, a common ratio is 1:20 or higher [8]. Key omega-3s including DHA (Docosahexaenoic acid) and EPA (Eicosapentaenoic Acid) are found in fish, flaxseed, walnuts, and avocados.
They foster
mental acuity,
a healthy nervous system,
immunity,
regular heart rhythm,
healthy heart growth, and
reduction in
inflammation,
blood clots,
serum triglycerides, and
LDL cholesterol [9].
Among the early work (2000) supporting the efficacy of Omega-3’s for dry eye, Carol Boerner, MD, followed 200 patients on 2,000 mg of flaxseed oil for three years. Symptoms improved in 85% [10]. An Association for Research in Vision and Ophthalmology (ARVO) presentation in 2003 by Trivedi, Sana, Gilbard, et al. summarized the Harvard Women's Health Study involving 39,876 patients. Results showed that the more tuna fish consumed, the lower the risk of dry eye: 2-4 servings/ week cut risk by 18% (compared to less than 2), and 5-6 servings/ week reduced risk by 66%. Not mentioned was the increased risk of mercury poisoning. In 2007 Athena Papas, DMD, et al. from Tufts University presented data at ARVO showed that utilizing an omega-3 supplement containing fish oil, flaxseed oil and vitamin E (Thera-tears Nutrition), resulted in significant reduction in symptoms of dry eye and dry mouth associated with Sjogren’s syndrome (61 patients). Another study presented at ARVO in 2012 and sponsored by Science Based Health analyzed administration of omega-3 and gamma linolenic acid (Hydro Eye) for 6 months in 38 postmenopausal women. Improvements were noted in patient’s symptoms (ocular surface disease index) and impression cytology inflammatory biomarkers, but no improvements were noted in corneal staining or tear breakup time.
A comparative study of three omega-3 preparations was reported by Frank Bucci, et al., at the American Academy of Ophthalmology meeting, 2011. This multicenter blinded randomized 3 month clinical study of 60 patients compared three oral supplements: PRN Dry Eye Omega Benefits, Nature made and Thera-tears [11]. Red blood cell membrane saturation index of Omega-3, EPA and DHA were measured [11]. The PRN preparation achieved desirable therapeutic levels of 8% after 1 month of use in 44% of patients, up from 4% at baseline; (measured by a simple finger stick blood test: Omega Quant, Sioux Falls, SD) [11]. Average values at 3 months were PRN 7.75%, Nature made 6.6%, and Thera-tears 5.9% [11].
All Omega-3 preparations are not created equal, relative to quality, purity and efficacy. One important difference is the chemical form finalized by the manufacturing process . The most pristine natural source of EPA and DHA is from pelagic fish in the Tasman Sea. Unfortunately, virtually all commercially obtained fish oil is contaminated by mercury and carcinogens. Processing requires the use of alcohol or ethyl ester to purify this mix, but two undesirable sequelae ensue.
The human body is poorly able to tolerate this foreign chemical alcohol leading to “fishy” side effects (dyspepsia) and perhaps more importantly, poor systemic absorption . For example a pill alleging 500 mg of omega-3 in the ethyl ester form may only deliver 200 mg. Furthermore, some OTC fish oil preparations in a water filled foam cup completely dissolve the cup bottom within several minutes. In order to remove the alcohol portion from the fish oil, a time consuming re-esterification process converts the product to its’ original triglyceride form. This has proven to yield superior absorption [12]. The desirable value of 8% is known to be cardio-protective. Achieving a significant serum level was noted in a study over 20 years ago to reduce the risk of sudden death by myocardial infarction by 90% [13]. Depending on a person’s weight and diet, an average dosage of 2 grams EPA and DHA daily for 2-3 months will likely achieve the desired level. Although flaxseed oil has some benefit due to abundant Omega-3’s, it also contains alpha linoleic acid. ALA is partially metabolized to arachidonic acid, a pro-inflammatory product.
Even with incomplete understanding of their mechanism of action, Omega-3 essential fatty acids were recommended as first line therapy by both the Dry Eye Workshop study group in 2007 and the International Workshop on Meibomian Gland Dysfunction in 2011 [14,15]. MGD is associated with altered lipid composition leading to increased tear evaporation and elevated tear osmolarity and subsequent ocular surface damage, epithelial cell desiccation, apoptosis and symptoms of burning and discomfort. High quality Omega-3 supplementation increases levels of unsaturated fatty acids in meibomian secretions which in a liquid state at room temperature prevent the blockage and stagnation within meibomian orifices. Thus tear film evaporation decreases, tear breakup time increases, and dry eye signs and symptoms improve. Additional benefits are decreased inflammation and increased tear secretion (by elevating CAMP).
An important feature of dry eye is inflammation and this condition, when associated with Omega-3 deficiency, can be linked to multiple other systemic illnesses . Many patients in the western world with dry eye also have age-related macular degeneration. In Japan these two conditions are virtually nonexistent due to a diet rich in Omega-3 EFA's **. Cardiovascular studies have shown strong benefits linking omega-3 ingestion with reduced risk of cardiovascular disease [16,17].
These benefits include
increased arterial elasticity,
decreased erythrocyte “stickiness”,
decreased arrhythmias,
decreased inflammation and
decreased serum triglycerides.
Young and middle aged patients with MGD have higher cholesterol levels than controls of similar age without MGD [18]. A 2016 study found that two large servings of oily fish / week reduced the risk of diabetic retinopathy by 48% [19]. Recent research has identified a new class of signaling molecules called resolvins. Derived from DHA and EPA, these compounds are necessary components of the endogenous system which acts as the “off-switch” for the normal inflammatory response [20].
Perhaps the most thorough and widely read study on the efficacy of omega-3’s appeared in Cornea, Sept., 2016, and analyzed the effects of a re-esterified triglyceride form in 105 patients [21]. This was a multicenter, prospective, interventional, placebo controlled, double masked study [21]. Subjects took 4 soft gels daily containing a total of 1680 mg of EPA/560 mg of DHA (Dry Eye Omega benefits, Physicians Recommended Nutraceuticals) or a control of 3136 mg of linoleic acid daily for 12 weeks [21].
The conclusion was a statistically significant improvement in each of five parameters measured:
Ocular Surface Disease Index score (patient's symptomatology),
tear osmolarity, MMP-9 (an inflammatory marker), o
mega-3 serum index levels, and
ear break up time [21].
Recent advances in knowledge regarding omega-3 essentials fatty acids will improve patient care both in dry eye disease and the rest of medicine. Two prescription oral omega-3 preparations are presently available: Lovaza (Omega-3-ethyl esters) and Vascepa (icosapent ethyl), a re-esterified triglyceride.* The great majority of OTC omegas-3’s are in the less desirable ethyl ester or alcohol form . A 2006 publication stated omega-3 deficiency or omeganemia was responsible for 96,000 deaths a yr. making it the sixth leading preventable cause of death in the United States *[22]. Regarding dry eye and multiple other conditions, the happier category of patients are those with mild-moderate disease who become asymptomatic with treatment [22]. All patients begin at stage one; it is more difficult and less satisfying to treat advanced disease.
Finally at least two* myths persisting about omega 3 essential fatty acids should be dispelled. First, patients on omega-3’s EFA’s are more prone to bleeding. This is true for most OTC brands due to the persistence of chemicals used to eliminate containments and pollutants. *When these chemical are removed, the re-esterified triglyceride form is both digestible and not associated with hematologic abnormalities. Second, one article linked Omega-3’s to prostate cancer [23]. This of course made national headlines
and the nightly news. Prior studies involving over 500,000 subjects have shown a reduction in prostate cancer. The study was seriously flawed in many ways and was later retracted [24]. Unfortunately, bad information was falsely sensationalized, and the correction never made the front page.
Dry eye has a high impact on quality of life due to discomfort and/or visual disability. In a typical eye care practice,* dry eye is the single most common complaint for patients seeking care . In both Dry Eye Workshop Study (DEWS) I & II reports from 2007 and 2017 respectively, nutritional therapy is listed as first line treatment for even mild dry eye. Evidence for benefits of nutritional supplementation continues to mount. Chinnery, et al. found that Omega-3 supplementation imparts neuroprotective effects in the cornea sub-basal plexus which correlate with improvement in tear osmolarity [25]. In another study, rosacea patients showed improvement in symptoms, *TBUT, Schirmer score and Meibomian gland score (MGS) with six months of Omega 3 supplementation [26]. An office-based study involving 1,419 patients in Spain found multiple benefits in dry eye sufferers utilizing a supplement that contained a combination of Omega-3 fatty acids, vitamins, minerals, and antioxidants [27].
A systematic review of fifteen independent studies involving 2,591 patients who used supplements with varying amounts of Omega-3 and Omega-6 EFA’s was published in March, 2017 [28]. Subjective symptom improvement was noted in seven of the studies and TBUT significantly increased in nine of the studies [28]. One reason for the variable results is the* variation in levels of Omegas in each supplement . While the AREDS II study failed to show statistical benefit for adding omega 3 EFA’s, it was most likely because the less desirable form (ethyl ester) and a suboptimal dose of 1 gram, (350mg DHA and 650mg EPA), were used [29]. The data is convincing that supplementation with high quality Omega-3 essential fatty acids (re-esterified triglyceride), in the proper dosage, is a starting point for treating this frustrating and potentially debilitating condition. References *1. Murphy, John J. Dry Eye Inflammation: A Discussion with Dr. Michael Lemp, MD Linx.com. 2017.
Cornea, Vol II, Krachmer, Mannis, Holland. 1997; 647.
Sullivan DA, Daniel Nelson J, Jennifer Craig P, Esen Akpek K, Dimitri Azar T, et al. TFOS DEWS II Introduction. 2017; 15: 269-275. Ref.: https://goo.gl/A6QsFp
Schiffman RM, Walt JG, Jacobsen G, Doyle JJ, Lebovics G, et al. Utility assessment among patients with dry eye disease. Ophthalmology. 2003; 110: 1412-1419. Ref.: https://goo.gl/P7Dexj
Farid M. The contribution of the tear film to vision and ocular comfort. Eyeworld. September, 2016: 6.
Moon JH, Kim KW, Moon NJ. Smartphone use in a risk factor for pediatric dry eye disease according to region and age. a case control study. BMC Ophthalmol. 2016; 16: 188. https://goo.gl/bUbcHc
Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of Aqueous deficient and Evaporative Dry Eye in a clinic Based patient Cohort: A retrospective Study. Cornea. 2012; 31: 472479. Ref.: https://goo.gl/ywiKyj
Simopoulos AP. Evolutionary aspects of diet, essential fatty acids and cardiovascular disease. Eur Heart J Supplements. 2001. Ref.: https://goo.gl/t7VxEh
Tribole E. The Ultimate Omega-3 Diet.
Boerner CF. Dry Eye successfully treated with oral flaxseed oil. Ocular Surgery News. 2000.
Bucci F, Kislan T. A Comparison of Omega-3 RBC Saturation for PRN-Dry Eye Omega Benefits V. Theratears Nutrition V. Nature Made. 2011.
Dyerberg J, Madsen P, Moller JM, Aardestrup I, Schmidt EB. Bioavailability of marine n-3 acid formulations. Prostaglandins leukotrienes essential fatty acids. 2010. 83: 137-141. Ref.: https://goo.gl/RpJrSL
Siscovick DS, Raghunathan TE, King I, Weinmann S, Wicklund KG, et al. Dietary Intake and Cell Membrane Levels of Long Chain Omega-3 Polyunsaturated Fatty Acids and the Risk of Primary Cardiac Arrest. JAMA. 1995; 274: 1363-1367. Ref.: https://goo.gl/9WC4JA
The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007; 5: 75-92. Ref.: https://goo.gl/Zxzocb
Nichols KK. The International Workshop on Meibomian gland Dysfunction. Invest Ophthalmol Vis Sci. 2011: 52: 1917-1921. Ref.: https://goo.gl/yr5m1t
Swanson D, Block R, Mousa SA. Omega-3 fatty acid EPA and DHA: Health Benefits throughout life. Adv Nutr. 2012; 3: 1-7. Ref.: https://goo.gl/fupSE4
Deckelbaum RJ, Torrejon C. The Omega-3 fatty acid nutritional landscape: Health Benefits and sources. J Nutr. 2012; 142: 587-591. Ref.: https://goo.gl/PUkswP
Pinna A, Blasetti F, Zinellu A, Carru C, Solinas G. Meibomian Gland Dysfunction and Hypercholesterolemia. Ophthalmology. 2013; 120: 2385-2389. Ref.: https://goo.gl/1dVLfu
Sala-Vila A, Dfaz-Lopez A, Valls-Pedret C, Cofan M, Garcfa-Layana A, et al. Dietary Marine Omega-3 Fatty Acids and Incident Sight Threatening Retinopathy in Middle Aged and Older Individuals with Type 2 Diabetes. JAMA Ophthalmol. 2016; 134: 1142-1149. Ref.: https://goo.gl/AjtE4s
Abelson MB, McLaughlin J. "Resolving” The effects of Fish Oil on the eye. Rev. Ophth. 2012; 74-77.
Epitropoulos AT, Donnenfeld ED, Shah ZA, Holland EJ, Faulkner WJ, et al. Effect of Oral Re- Esterified Omega-3 Nutritional Supplementation on Dry Eyes. Cornea. 2016; 35: 1185-1191. Ref.: https://goo.gl/P6apTE
Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, et al. The Preventable Cause of Death in the United Sates: Comparative Risk Assessment of Dietary, Lifestyle and Metabolic Risk Factors. PLOS Med. 2009. Ref.: https://goo.gl/Cd2fBE
Brasky TM, et al., Nutr Cancer, 2011, doi: 10.1080/01635581.2011.553022
White D, Study sends wrong message about Omega-3 fatty acids and prostate cancer. Ocular Surgery News, 3/25/2014, 8.
Chinnery HR, Naranjo Golborne C, Downie LE. Omega-3 supplementation is neuroprotective to corneal nerves in dry eye disease: a pilot study. Ophthalmic Physiol Opt. 2017; 37: 473-481. Ref.: https://goo.gl/EwvBXW
Bhargava R, Mini Chandra, Utsav Bansal, Divya Singh, Somesh Ranjan. A Randomized Controlled Trial of Omega 3 Fatty Acids in Rosacea Patients with Dry Eye Symptoms. Current Eye Research. 2016. https://goo.gl/oH5PzU
Gatell-Tortajada J. Oral supplementation with a nutraceutical formulation containing omega-3 fatty acids, vitamins, minerals, and antioxidants in a large series of patients with dry eye symptoms: results of a prospective study. Clin Interv Aging. 2016; 11: 571-578. Ref.: https://goo.gl/8JUrAL
Molina-Leyva I, Molina-Leyva A, Bueno-Cavanillas A. Efficacy of nutritional Supplementation with omega-3 and omega-6 fatty acids in dry eye syndrome: a systematic review of randomized clinical trials. Acta Ophthalmol.2017; 95: 677-685. Ref.: https://goo.gl/FhTnfj
Age-Related Eye Disease Study Protocol.
3,000 mg of Omega-3 for a year helped a bit more than oilve oil placebo- April 2018* n−3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease New England Journal Of Medicine DOI: 10.1056/NEJMoa1709691 📄 Download the PDF from VitaminDWiki *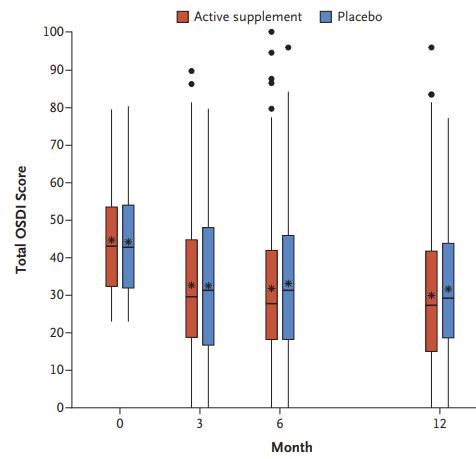
BACKGROUND
Dry eye disease is a common chronic condition that is characterized by ocular discomfort and visual disturbances that decrease quality of life. Many clinicians recommend the use of supplements of n−3 fatty acids (often called omega-3 fatty acids) to relieve symptoms.
METHODS
In a multicenter, double-blind clinical trial, we randomly assigned patients with moderate-to-severe dry eye disease to receive a daily oral dose of 3000 mg of fish-derived n−3 eicosapentaenoic and docosahexaenoic acids (active supplement group) or an olive oil placebo (placebo group). The primary outcome was the mean change from baseline in the score on the Ocular Surface Disease Index (OSDI; scores range from 0 to 100, with higher scores indicating greater symptom severity), which was based on the mean of scores obtained at 6 and 12 months. Secondary outcomes included mean changes per eye in the conjunctival staining score (ranging from 0 to 6) and the corneal staining score (ranging from 0 to 15), with higher scores indicating more severe damage to the ocular surface, as well as mean changes in the tear break-up time (seconds between a blink and gaps in the tear film) and the result on Schirmer’s test (length of wetting of paper strips placed on the lower eyelid), with lower values indicating more severe signs.
RESULTS
A total of 349 patients were assigned to the active supplement group and 186 to the placebo group; the primary analysis included 329 and 170 patients, respectively. The mean change in the OSDI score was not significantly different between the active supplement group and the placebo group (−13.9 points and −12.5 points, respectively; mean difference in change after imputation of missing data, −1.9 points; 95% confidence interval [CI], −5.0 to 1.1; P=0.21). This result was consistent across prespecified subgroups. There were no significant differences between the active supplement group and the placebo group in mean changes from baseline in the conjunctival staining score (mean difference in change, 0.0 points; 95% CI, −0.2 to 0.1), corneal staining score (0.1 point; 95% CI, −0.2 to 0.4), tear break-up time (0.2 seconds; 95% CI, −0.1 to 0.5), and result on Schirmer’s test (0.0 mm; 95% CI, −0.8 to 0.9). At 12 months, the rate of adherence to treatment in the active supplement group was 85.2%, according to the level of n−3 fatty acids in red cells. Rates of adverse events were similar in the two trial groups.
CONCLUSIONS
Among patients with dry eye disease, those who were randomly assigned to receive supplements containing 3000 mg of n−3 fatty acids for 12 months did not have significantly better outcomes than those who were assigned to receive placebo. (Funded by the National Eye Institute, National Institutes of Health; DREAM ClinicalTrials.gov number, NCT02128763.)
Dry eye after LASIK surgery treated by Vitamin D - RCT MAY 2022* Oral vitamin D 3 supplementation for femtosecond LASIK-associated dry eye vitamin D for LASIK dry eye syndrome *Int Ophthalmol . 2022 May 12. doi: 10.1007/s10792-022-02314-5 PDF costs $40
Ying Lin 1, Huanjun Su 1, Jianbin Wu 2, Muzhi Yuan 1, Yong Zhang 3
Purpose: To assess the effect of oral vitamin D3 supplementation in dry eye after femtosecond laser-assisted in situ keratomileusis (FS-LASIK).
Setting: Liuzhou Worker's Hospital.
Design: This prospective study included 90 patients selected between January and December in 2019, who underwent FS-LASIK operation in our hospital and had obvious symptoms indicating dry eyes 1 month after operation. The subjects were randomly divided into two groups: The experimental group (n = 45) received* vitamin D3 2000 IU/D continuously for 12 weeks *; the control group (n = 45) did not take vitamin D3 orally. Ocular surface disease index (OSDI), Tear breakup time (TBUT) and Schirmer's test I were evaluated premedication and 1,3,6 months after treatment. Serum vitamin D3 level and the mean concentration of cytokine IL-6, IL-17, IL-23 in t ears were also measured.
Results: One month after treatment, the mean OSDI score of the
experimental group (11.67 ± 8.53) was significantly lower than that of the
control group (23.82 ± 13.22) (P = 0.007).
TBUT (10.71 ± 1.02 s) and Schirmer I (9.36 ± 0.40 mm) of the experimental group were higher than those of the control group (7.49 ± 1.29 s and 7.51 ± 0.44 mm). The OSDI (10.25 ± 5.49) was significantly lower than those of the control group(20.22 ± 6.23) and TBUT (10.75 ± 1.09 s) and Schirmer I test value (11.34 ± 0.39 mm) of the experimental group were significantly higher than those of the control group (8.36 ± 1.23, 8.12 ± 0.50) at 3 months after treatment. There were significant differences in OSDI, TBUT (P < 0.05) and Schirmer I test value between the two groups at 6 months after treatment. Serum vitamin D3 level was negatively correlated with OSDI score (r = - 0.90; P = 0.00) and positively correlated with Schirmer I test (r = 0.88; P = 0.00), TBUT score (r = 0.89; P = 0.00) and TMH (r = 0.80; P = 0.00). IL-17 level was shown to be significantly correlated with TBUT(r = - 0.25, P = 0.014) and Schirmer I test (r = - 0.21, P = 0.018). IL-6 level was significantly correlated with OSDI (R = 0.18, P = 0.020) and TBUT (R = 0.20, P = 0.019).
See also web
- What is Dry Eye Syndrome? + 20 Incredible Facts 2017?** A great many products for Dry Eye are based on Omega-3 (2017)
 126 products ("dry eye" Omega-3_ were on Amazon as of Sept 2024__
126 products ("dry eye" Omega-3_ were on Amazon as of Sept 2024__
1. There have been <span style="color:#00F;"><!-- {SQL(db=>vitamind)}SELECT hits FROM tiki_pages WHERE page_id=9165{SQL} --></span> visits to this page