Web update May 2016
- What Is The Best Magnesium Supplement? A Comprehensive Review 2016?
Dietetian decided Citrate and Gluconate were best
Reviews Oxide, Oxalate, Gluconate, Citrate, Chloride, Hydroxide. Aspartate, Glycinate, Orotate, L-Threonate
From http://suppversity.blogspot.com/
Magnesium Round-Up: Know If You Are Deficient, Whether You Need More, Where to Find It, How Dietary Mg Contents Changed & How it Interacts W/ Vitamin D audio

|
| 24%, 23% and 22% of the DV for magnesium that's what you can find in one serving of sunflower seeds (0.25cup), halibut (4oz) and a large(r) banana - now you tell me it was impossible to get your magnesium from dietary sources. |
After having handled half of the Science Round-Up from Thursday yesterday, yesterday, there is still something left to serve: seconds to the seconds, if you will and probably not so "new" as the average SuppVersity news. In order not to bore you, I will yet refrain from telling you how important magnesium is and how it is involved in thousands of enzymatic reactions ... you know the whole magnesium-guru-spiel all too well, anyway. I mean, anyone doing a cursory Google search will have to conclude that there is nothing magnesium cannot cure, right?. Whatever you may suffer from, someone has already found out that it must be related to magnesium deficiency or, even more profitable, taking the wrong form of magnesium supplements.
Apropos deficiency: How do you even know you are deficient?
What sounds like a question that could be answered in one, at best two sentences turns out to be one of the root causes of the whole confusion about magnesium. Based on a standard blood test you can only exclude that your levels are (a) so high or (b) so low that you better head straight to the emergency room. Magnesium is, just as the other electrolytes, simply too important for your body to have them drop below a certain margin in which your heart works optimally. So if there is not enough magnesium around, your body will tap into tissue stores the status of which is obviously not identical to the serum levels on a standard lab test.
|
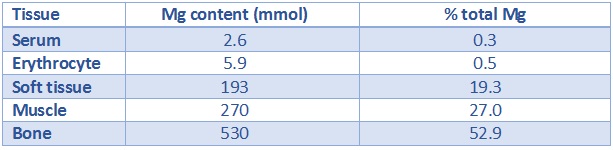
| Table 1:The lion's share of magnesium to replete your serum levels is not coming from your red blood cells and therefore RBC levels are only a proxy and not a 100% reliable marker of total body mg status (data based on Elin. 1987) |
According to Maurice J. Arnaud who wrote a review with the telling title "Update on the assessment of magnesium status" in 2008, the most reliable method to assess the whole body magnesium status would be a metabolic ward study in the course of which a so-called "loading test" would be performed, But...
"balance studies are time consuming, labour intensive and need well trained staff. They are often performed in a metabolic unit and require complete urine and faecal collections; therefore it is not a method that can be applied as a routine test for the evaluation of Mg status. Loading tests are simplified balance studies where absorption is supposed not to be disturbed when Mg is given orally so that body retention is calculated from urine elimination. Mg administration during a loading test can be either oral or intravenous and it is important that the subjects have normal kidney function. Urine is collected for 24 hours following administration of the Mg load as Mg excretion by the kidney has been shown to have a circadian rhythm . Under these conditions, the loading test is supposed to be a reliable indicator of Mg status." (Arnaud. 2008)
With the erythrocyte (red blood cell) test for magnesium, there is however an alternative available, which may not be just as reliable but appears to show a relatively high correlation with whole body magnesium levels in many, but not all studies (Malon. 2004).
How likely is it that you are deficient?
Honestly, I would hope that it is unlikely, because if that is the case for someone who is not taking supplemental magnesium you can almost be sure that her or she is following a healthy whole foods diet.
|
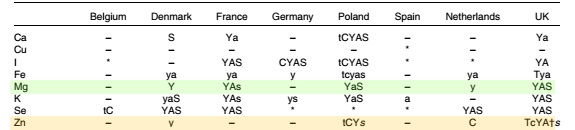
| Table 2: Overview of age groups with more than 5 % of intakes below the lowest recommended intake levels in 7 European countries; T, toddlers (1–3 years (both sexes)); C, children (4–10 years); Y, youth (11–17 years); A, adults (18–60 years); S, seniors (.60 years); capitals, both sexes; lower case, women only; lower case italic, men only (Mensik. 2013) |
If you take a look at table 2 you will see that even the average German gets enough magnesium in his diet, irrespective of his age, and much contrary to our neighbors in the East, West and Northwest (I could not resist to mark zinc another of those purported minerals of which conventional wisdom tells you that you simply cannot get enough from your diet).
Knowing that most of you are probably Americans, I can calm you down. You are not worse than your British friends. In fact, the NHANES data from 1999-2000 suggests that the average American Caucasian and Mexican man below 50 gets enough magnesium from his food only! Unfortunately, the same cannot be said for the women, and both male and female African Americans who have trouble meeting their requirements even if one accounts for the additional magnesium from supplements (NHANES).
Magnesium and the athlete
A note on magnesium and cramps: While there is evidence that altered serum osmolality and altered serum electrolyte concentrations, notably hypochloraemia, hyponatraemia, and hypocalcaemia (=not hypomagnesaemia) can cause generalized skeletal muscle cramping at rest in specific clinical settings, "data from well-conducted prospective cohort studies show that athletes with acute EAMC are not hyponatraemic, hypochloraemic, or hypocalcaemic and do not have an abnormal serum osmolality." (Schwellnus. 2008).
For the average athlete, a low magnesium intake is yet rather the exception. It is thus no wonder that not magnesium deficiencies, but high magensium levels are a problem that is commonly observed in athletes. I mean, what are you supposed to do, when even your mother "lies" to you about cramps being caused by magnesium deficiency?
"The most common alterations were higher serum phosphate (29/61, 47%) and magnesium concentrations (28/61, 46%). Abnormalities of serum phosphorus and magnesium concentrations were detected in almost half of the athletes. Hyperphosphataemia and hypermagnesaemia were the most common abnormalities." (Malliaropoulos. 2012)
The data Malliaropoulos et al. analyzed came from 130 elite track and field athletes (65 males and 65 females, age range 20-30 years) from the National Athletics Sports Medicine Center database in Thessaloniki, Greece. And maybe some of them were even on the proven non-ergogenic ZMA (zinc + magnesium + vitamin B6; cf. Wilborn. 2004)
So where do you get your supplemental magnesium from and how much?
I am not going to tell you to stop supplementing with magnesium if you feel that this has done you good in the past. It is after all an important mineral. What I want to remind you of is yet the fact that taking 100% of the RDA is imho the absolute maximum. Even if you don't end up with high levels due to supplementing more and don't care about wasting money, there is one thing that's commonly overlooked about human physiology and that is how the intake and excretion of nutrients are highly inter-related. In other words, if your body switches into a "get rid of magnesium" mode it is likely you are loosing other electrolytes you do not supplement in copious amounts (e.g. salt ;-), as well.
|
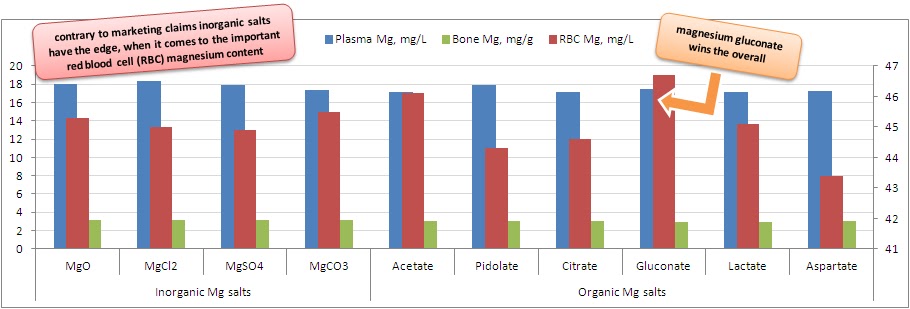
| Figure 1: Plasma an bone (primary axis) as well as red blood cell (RBC; 2ndary axis(!)) content after 14 days of supplementation with identical amounts of magnesium in different organic and inorganic forms (Coudray. 2005) |
Coudray PDF is attached at the bottom of this page
As far as the best forms are concerned the number of studies comparing multiple forms to each other is limited and the inter-comparison of different studies not really legit. Therefore I have simply copied + pasted the figure that went with a previous article on the matter - as you can see, you can generally use whatever form of magnesium you want - even the cheap oxides, which worked wonders for anxiety ridden ladies in a study by De Souza et al. that was published in the Journal of Women's Health & Gender-Based Medicine in March 2000. As long as you take your magnesium supplements in reasonably low doses - the dose in the De Souza study for example was 200mg + 50mg B6 - and over a long enough period, they are going to bring your levels back up - if not sooner, then later.
Magnesium depletion of our foods
A note on topical Epsom salt from the early 20th century: While I did tell you on the show that I could not find peer-reviewed adequately powered studies on the topical absorption of magnesium in the for of mg oil or Epsom salt, I found a comment in a 1915 paper on the potential harm caused by cosmetics quite enlightening, esp. the part on the economic value of respective products, where Martin I. Wilber writes that the ability of respective products to penetrate the "unbroken skin has as yet not been demonstrated" and cautions against the sue "of the now widely advertised lotions containing magnesium sulphate or Epsom salt", of which "the latter preparations serve very well to show the gullability of that portion of the public that is desirous of improving its facial appearance. As Epsom salt, magnesium sulphate can usually be purchased for 5 cents a pound, while in the form of any one of the popular skin or wrinkle lotions it is sold at the rate of from $2 to $4 a pound." (Wilbert. 1915) You see, there were snake,... ah I mean mg oil vendors all over the place even 100 years ago ;-)
Aside from the almost cult-like worship of epsom salt baths and topical ng oils, the notion of a general depletion of mg in the foods we eat is one of the favorites among the bazillion of websites run by people who hoax you to believe they were concerned with your physical health, when all they are concerned with is their own financial health.

|
| Figure 2: Changes in mineral content of selected food types from 1940-2002 (Thomas. 2007) |
It is, as the data in figure 2 goes to show you true that the amount of magnesium in many of the foods we consume is lower these days than it was amidst WW2. The mg loss in meats, for example, is driven by the processing, while corned beef has lost almost 50% of its "original" mg content, the amount of mg in roast beef and steaks is still the same, the one in turkey is even up by ~30% and for chicken it remained 100% stable (Thomas. 2007). It is also a very intriguing coincidence that the same websites will usually also tell you how we are all not just magnesium deficient, but also copper toxic. Strange in view of the fact that the average reduction in copper is -62% and thus >2x higher than that of magnesium.
Magnesium supplementation for special conditions
Before closing this round-up with a bottom line, I am briefly listing a couple of things related to magnesium or rather a deficiency in this important mineral that could be solved by simply upping your dietary and/or supplemental magnesium intake.

|
| Higher vitamin D levels increase MG uptake from the gut and supplementation with VD has been shown to increase mg in obese, yet not in normal individuals (Farhanghi. 2009). On the other hand, mg has recently been found to be necessary for the production of calcitriol from 25OHD (Matsuzaki. 2013) |
- depression - low cellular mg levels can precipitate if not cause depression(-like) symptoms, 150-300mg of magnesium glycinate or better taurinate can help (Eby. 2006)
- low vitamin D - while it is not yet sure if it helps with upping the storage form of vitamin D (25OHD), it has been recently established that magnesium is necessary for the production of calcitriol the active form of vitamin D; adequate levels of D also facilitate mg absorption very high levels of vitamin D, on the other hand, have been associated with low / imbalanced mg levels - probably due to their effects on calcium homestasis
- constant stress / burnout - initially low mg levels will lead to a hyper activity of the stress-axis within the HPTA; the constantly overtaxed CNS will then give in and you will end up totally burned out (Sartori. 2011); this state cannot be reversed by magnesium supplementation, alone, but it can aid the recovery process which is largely based on taking off of everything that stresses you
Whether or not simply eating more high magnesium foods will be enough or whether you actually have to buy supplements to work on these and other issues will also depend on whether
- you can digest / absorb it, which would be hampered due to vomiting, diarrhea, bowel resection, intestinal and biliary fistulas or hemorrhagic pancreatitis
- lose too much mg over the kidneys, due to chronic parental fluid therapy, osmotic diuiresis, hypercalcemia, diuretics, aminoglycosides, amphotericin B, pentamidine, cisplatin, cyclosporine, alcohol metabolic acidosis (ketosis, starvation, alcoholism), renal diseases, or
- suffer from endocrine disorders like primary or secondary aldosteronism, diabetes, hyperthyroidism or hyperparathyroidism
If anything of these sounds familiar, I would certainly consider testing my mg levels (erythrocyte test) before and while I was supplementing and that's not about wasting money on potentially unnecessary supplements, but much more about making sure that you actually get, absorb and retain enough magnesium.
Bottom line: Magnesium is certainly an important mineral, but its effects must not be seen in isolation, it should not be supplemented in copious amounts in isolation without medical indication and it may not be misunderstood as a natural pharmacological agent - it works by (a) replacing a deficiency or (b) countering an imbalance. Plus: It is not generally impossible to get your 300-400mg of magnesium from your diet.
References:
- Arnaud MJ. Update on the assessment of magnesium status. Br J Nutr. 2008 Jun;99 Suppl 3:S24-36.
- Bohl CH, Volpe SL. Magnesium and exercise. Crit Rev Food Sci Nutr. 2002;42(6):533-63. Review.
- Miriam C. De Souza, Ann F. Walker, Paul A. Robinson, and Kim Bolland. Journal of Women's Health & Gender-Based Medicine. March 2000, 9(2): 131-139.
- Eby GA, Eby KL. Rapid recovery from major depression using magnesium treatment. Med Hypotheses. 2006;67(2):362-70.
- Elin RJ. Assessment of magnesium status. Clin Chem. 1987 Nov;33(11):1965-70. Review.
- Farhanghi MA, Mahboob S, Ostadrahimi A. Obesity induced magnesium deficiency can be treated by vitamin D supplementation. J Pak Med Assoc. 2009 Apr;59(4):258-61.
- Malliaropoulos N, Tsitas K, Porfiriadou A, Papalada A, R Ames P, Del Buono A, Lippi G, Maffulli N. Blood phosphorus and magnesium levels in 130 elite track and field athletes. Asian J Sports Med. 2013 Mar;4(1):49-53.
- Malon A, Brockmann C, Fijalkowska-Morawska J, Rob P, Maj-Zurawska M. Ionized magnesium in erythrocytes--the best magnesium parameter to observe hypo- or hypermagnesemia. Clin Chim Acta. 2004 Nov;349(1-2):67-73.
- Matsuzaki H, Katsumata S, Kajita Y, Miwa M. Magnesium deficiency regulates vitamin D metabolizing enzymes and type II sodium-phosphate cotransporter mRNA expression in rats. Magnes Res. 2013 May 1;26(2):83-6.
- Mensink GB, Fletcher R, Gurinovic M, Huybrechts I, Lafay L, Serra-Majem L, Szponar L, Tetens I, Verkaik-Kloosterman J, Baka A, Stephen AM. Mapping low intake of micronutrients across Europe. Br J Nutr. 2013 Aug;110(4):755-73.
- Sartori SB, Whittle N, Hetzenauer A, Singewald N. Magnesium deficiency induces anxiety and HPA axis dysregulation: modulation by therapeutic drug treatment. Neuropharmacology. 2012 Jan;62(1):304-12. doi: 10.1016/j.neuropharm.2011.07.027. Epub 2011 Aug 4.
- Schwellnus MP. Cause of exercise associated muscle cramps (EAMC)--altered neuromuscular control, dehydration or electrolyte depletion? Br J Sports Med. 2009 Jun;43(6):401-8.
- Thomas D. The mineral depletion of foods available to us as a nation (1940-2002)--a review of the 6th Edition of McCance and Widdowson. Nutr Health. 2007;19(1-2):21-55. Review.
- Wilbert MI. Cosmetics as Drugs: A Review of Some of the Reported Harmful Effects of the Ordinary
Constituents of Widely Used Cosmetics. Public Health Reports. 1896-1970; 30(42): Oct. 15, 1915. 3059-3066. - Wilborn CD, Kerksick CM, Campbell BI, Taylor LW, Marcello BM, Rasmussen CJ, Greenwood MC, Almada A, Kreider RB. Effects of Zinc Magnesium Aspartate (ZMA) Supplementation on Training Adaptations and Markers of Anabolism and Catabolism. J Int Soc Sports Nutr. 2004 Dec 31;1(2):12-20.
See also VitaminDWiki
- Magnesium compounds have similar bioavailability when integrated in food – Dec 2005 Coudray study referenced above