Perhaps 4X more likely to die of COVID-19 if take ACE inhibitors (reduce blood pressure)
DR. MALCOLM KENDRICK post 22nd March 2020
( Bolding added by VitaminDWiki)
I thought I should do a quick update on COVID-19, as some interesting and important information has been published in Italy. Looking at deaths in various age groups, underlying conditions etc.
It can be seen here https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-201920marzo_eng.pdf
Points of greatest importance
Far more men are dying than women, with a ratio of around 3:1 – reasons unknown
Mean age at death is 78.5 years (women slightly older than men)
2% of those dying had no comorbidities (other diseases e.g. heart disease, diabetes, cancer)
~50% had three or more comorbidities.
Symptoms
1% were coughing up blood (haemoptysis)
8% had diarrhoea
40% had a cough
73% had difficulty breathing (dyspnoea)
76% had a fever.
[5.7% were admitted with no symptoms at all – not clear what they came in with.
Presumably admitted with something else, then developed the symptoms later]
What did they die of?
96.5% died of acute respiratory distress syndrome.
‘Acute respiratory distress syndrome (ARDS) occurs when fluid builds up in the tiny, elastic air sacs (alveoli) in your lungs. The fluid keeps your lungs from filling with enough air, which means less oxygen reaches your bloodstream. This deprives your organs of the oxygen they need to function.
ARDS typically occurs in people who are already critically ill or who have significant injuries. Severe shortness of breath — the main symptom of ARDS — usually develops within a few hours to a few days after the precipitating injury or infection.
Many people who develop ARDS don’t survive. The risk of death increases with age and severity of illness. Of the people who do survive ARDS, some recover completely while others experience lasting damage to their lungs.’1
Treatment is with oxygen and ventilation but has a low success rate in the very elderly.
Deaths under 50 years of age
To date (March the 20th), 36 of 3200 (1.1%) COVID-19 positive patients under the age of 50 have died. In particular, 9 of these were younger than 40 years, 8 men and 1 woman (age range between 31 and 39 years). For 2 patients under the age of 40 years, no clinical information is available; the remaining 7 had serious pre-existing pathologies (cardiovascular, renal, psychiatric pathologies, diabetes, obesity).
There do not seem to have been any deaths below the age of thirty.
ACE-inhibitors and Angiotensin Receptor Blockers (ARBs)
There has been much debate as to whether or not ACE-inhibitors (angiotensin converting enzyme inhibitors) and ARBs may increase the risk of death [these drugs are widely used to lower blood pressure]. This is because COVID-19 appears to enter the body through ACE2 receptors – found in high concentrations in the lungs and can cause upset to the neurohormonal system where ACE, and ACE receptors, play an important role.
The data from Italy is that:
‘Before hospitalization, 36% of COVID-19 positive deceased patients followed ACE-inhibitor therapy and 16% angiotensin receptor blockers-ARBs therapy. This information can be underestimated because data on drug treatment before admission were not always described in the chart.’
That is 52% who were on one, or the other (it is very rare for anyone to be on both). That was clearly, as they state, an underestimate. Possibly a considerable underestimate.
Knowing this, it is important to know how many (elderly people) take either of these drugs, to see if there is a correlation between taking them and dying from COVID-19. The figures from Italy are not clear at all. However, the latest data on prevalence of high blood pressure in the adult Italian population was, around 52% (This is an absolute maximum).2
However, the number of people known to have had their high blood pressure recorded by their general practitioner is around 20% 3 . Which means that most people with high blood pressure are not treated with anything.
Bringing these figures together, it can be estimated that a maximum of 10% of the Italian population are taking antihypertensive medications. These figures may be a little out of date, and these data are not specifically for the age group of, around, 80 years of age. Here the figures on diagnosis of hypertension, and use of antihypertensives will probably be higher, possible double.
So, we can say that 10% of the adult population is treated for hypertension, and that this may be around 20% in those aged around 80. Taking the figures one step further, it is estimated that about 67% of those who take antihypertensive in Italy use ACE-inhibitors, or ARB. 4
Bringing all of these figures together, it is likely the average percentage of eighty-year olds taking an ACE, or ARB is
67% of 20% of 52%x 2 = 14.0%
Which means that amongst 80-year olds ~14% are taking one, or other, of these drugs.
I cannot say either of these figures in carved in stone and I believe 14% is probably a overestimate. I wish there were more fully accurate figures to be had. So, what does this mean?
It means that:
A (probable) maximum of 14% of the elderly population in Italy are taking ACE-inhibitors/ARBs
A minimum of 52% of people in Italy who are dying from COVID-19 are taking ACE-inhibitors/ARBs.
Which suggests you are four times as likely to die from COVID-19 if you are taking one of these drugs, prior to contracting the virus. This, of course, does not take into account confounding variables – many of which are currently unknown. By a confounder I mean that people taking these drugs may have more comorbidities, such as heart disease, diabetes etc.
However, it remains a very strong signal, and I do not think it can be ignored, particularly in the light of the knowledge that the COVID-19 virus has a significant impact on the ‘ACE system’.
On this basis I would strongly recommend that elderly people, with any comorbidity, who is taking an ACE-inhibitor/ARB should look to change their antihypertensive treatment to something else – whilst the threat from COVID-19 is high.
I should point out this runs contrary to the advice from the authors of a study in the European Heart Journal 20th March:
SARS-CoV2: should inhibitors of the renin–angiotensin system be withdrawn in patients with COVID-19?
‘In conclusion, based on currently available data and in view of the overwhelming evidence of mortality reduction in cardiovascular disease, ACE-I and ARB therapy should be maintained or initiated in patients with heart failure, hypertension, or myocardial infarction according to current guidelines as tolerated, irrespective of SARS-CoV2. Withdrawal of RAAS inhibition or preemptive switch to alternate drugs at this point seems not advisable, since it might even increase cardiovascular mortality in critically ill COVID-19 patients.’ https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehaa235/5810479
It should be borne in mind though, that their advice does acknowledge that they had no evidence about the number of people who were taking ACE-inhibitors, or ARBs, who then died. The data from Italy came out a day after the EHJ article was published.
Of course, no-one can be certain about what exactly is happening. I cannot be certain, but the signal from Italy on ACE-inhibitors and ARBs, seems very strong, and concerning. Based on it, I think my advice would be to change medication, if possible.
Stating this, I am aware that most GPs will not change anything, unless they get instruction from the acknowledged experts. Unfortunately, this is likely to take far more time than many people actually have.
See also VitaminDWiki
{include}
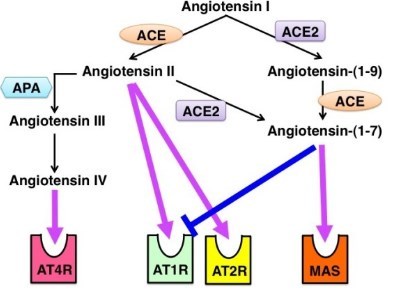
Coronaviruses attach to cells via ACE2, Vitamin D might reduce ACE2 has the following diagram

ACE and ACE2 functions