Breast Cancer prevented by Vitamin D (most studies concur)
Vitamin D and Breast Cancer: Latest Evidence and Future Steps
Breast Cancer: Basic and Clinical Research Volume 11: 1-8 © The Author(s) 2017 DOI: 10.1177/1178223417749816
 click on image for details
1. Treatment of Breast Cancer by Vitamin D as well – other studies
* Cancer survival 4 percent more likely with just a little more vitamin D (4 ng) - meta-analysis July 2014
* Vitamin D after breast cancer diagnosis - May 2012
* Vitamin D and breast cancer radiation
* Breast Cancer Mortality reduced 60 percent if more than 60 ng of Vitamin D – meta-analysis June 2017
* More survive Breast Cancer if more vitamin D – 2X fewer deaths with just 30 ng -meta-analysis March 2014
click on image for details
1. Treatment of Breast Cancer by Vitamin D as well – other studies
* Cancer survival 4 percent more likely with just a little more vitamin D (4 ng) - meta-analysis July 2014
* Vitamin D after breast cancer diagnosis - May 2012
* Vitamin D and breast cancer radiation
* Breast Cancer Mortality reduced 60 percent if more than 60 ng of Vitamin D – meta-analysis June 2017
* More survive Breast Cancer if more vitamin D – 2X fewer deaths with just 30 ng -meta-analysis March 2014
📄 Download the PDF from VitaminDWiki
Manar Atoum manar@hu.edu.jo and Foad Alzoughool
Department of Medical Laboratory Sciences, Faculty of Allied Health Sciences, The Hashemite University, Zarqa, Jordan
Vitamin D (the sunshine vitamin) plays a vital role in calcium homeostasis, skeletal metabolism, and immune, cardiovascular, and reproductive systems’ functions. The worldwide prevalence of vitamin D deficiency is approximately 1 billion. Vitamin D deficiency is a serious health problem with numerous health consequences; it is associated with diabetes, rheumatic arthritis, Parkinson, Alzheimer diseases, osteomalacia, osteoporosis, and fractures in adults and cancers. Many reports showed an inverse association between serum vitamin D concentration and incidence of several cancers, including breast, colorectal, kidney, lung, and pancreatic. About 20 different cancers have incidence rates inversely related to solar UV-B doses and serum vitamin D concentration. Considering the rising incidence of breast cancer and high prevalence of vitamin D deficiency, this review aimed to reflect an association between serum vitamin D concentration and breast cancer risk, reveal the link between vitamin D receptor genetic polymorphisms and breast cancer risk, and review the relationship between vitamin D level, breast cancer risk, and prognostic factors such as tumor stage, grade, size, lymph node involvement, and hormone receptor status.
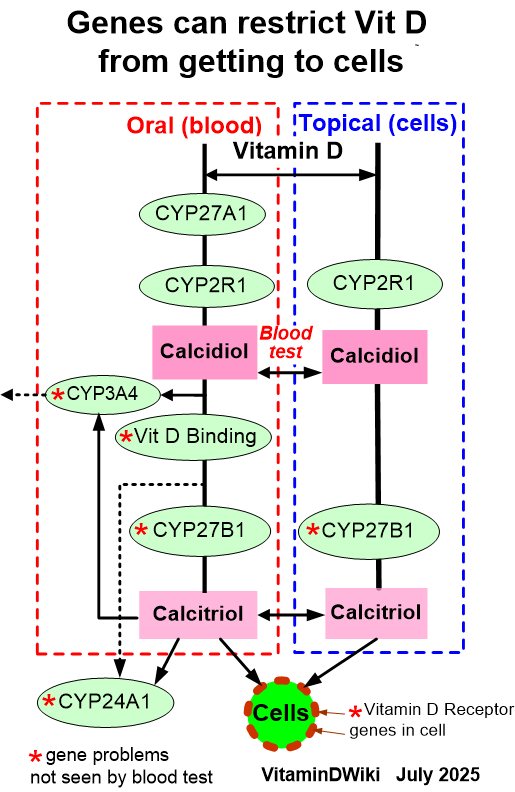
Vitamin D refers to a group of fat-soluble secosteroids that are produced in 2 forms: D2 and D3. The D3 form is produced from 7-dihydroxycholesterol under the skin that is exposed to UV-B light (cholecalciferol) and D2 form originates from dietary sources such as plants and fish (ergocalciferol). Most of the vitamin D (up to 90%) comes from endogenous production under the skin. Both forms undergo hydroxylation in the liver by mitochondrial and microsomal 24-hydroxylase (encoded by CYP24A1) to yield 25-hydroxyvitamin D (25(OH)D) or cal- cidiol. The 25(OH)D is then transported in the circulation by the vitamin D-binding protein and further metabolized in kidneys to produce 1,25 dihydroxyvitamin D (1,25(OH)2D) (by 101-hydroxylase that is encoded by CYP27B1) or calcitriol. The half-life of 1,25(OH)2D is only 4 to 6 hours and 1000-fold less than the total 25(OH)D. So, serum vitamin D is usually determined by measuring 25(OH)D biomarker that has a half-life of about 2 to 3 weeks.1
Different medical societies’ guidelines have different definitions for the cutoff values of vitamin D level. The Institute of Medicine guidelines suggest that individuals are at risk of vitamin D deficiency if 25(OH)D concentration is below 30 nmol/L, inadequacy at serum 25(OH)D concentration between 30 and 50 nmol/L, and individuals are considered sufficient at concentration 50 nmol/L or higher.2 In contrast, the Endocrine Society guidelines defined that 50 nmol/L is a cutoff value for vitamin D deficiency and the sufficient concentration exceeds 75 nmol/L.3
Breast cancer has been considered as the most common type of cancer among the women within 161 countries, and the **most common cause for cancer deaths, within 98 countries.4
Known and well-established risk factors for breast cancer include age, family history, the density of breast tissue, parity, overweight, alcohol intake, and genetic risk factors such as BRCA mutations.5 Recently, vitamin D* receptor ( VDR ) genes were reported to increase breast cancer risk.6 Several molecular breast cancer subtypes have been identified: luminal A and B (accounting for 50%-60% of breast cancer cases), basal-like or triple-negative (10%-20% of breast cancer cases) and human epidermal growth factor receptor 2 (HER2)-enriched (10%- 15% of cases).7 Vitamin D receptor *genes operated by vitamin D have important roles in the mammary gland through regulation of calcium transport during lactation, hormone differentiation, and milk production.8 Many efforts and enormous research have been directed toward identifying vitamin D as a breast cancer risk factor to be targeted for cancer prevention. This is because circulating vitamin D levels (levels >45 ng/mL) may protect against breast cancer9 and because breast cancer chemoprevention drugs that alternate the carcinogenesis process such as estrogen receptor modulators, tamoxifen, raloxifene, and aromatase inhibitor have high toxicities and not effective in the aggressive estrogen receptor-negative (ER-) breast cancers.10
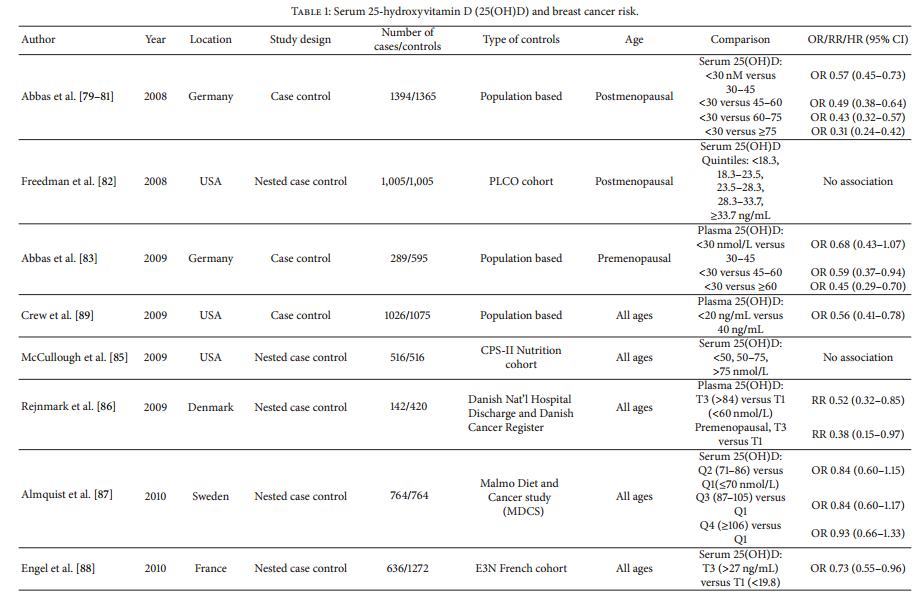
Many studies examined the association between vitamin D level and breast cancer risk, which generally show an inverse association (Table 1). The meta-analysis conducted by Chen et al11 revealed that women with the highest quantile of circulating 25(OH)D was associated with a 45% (odds ratio [OR] = 0.55, 95% confidence interval [CI] = 0.38-0.80) decrease in breast cancer risk when compared with those women with the lowest quantile of blood 25(OH)D.
Table 1. Studies examined the association between vitamin D and breast cancer risk.
Another meta-analysis of nested case-control studies found a step-wise inverse association beyond a threshold of 27 ng/mL, but with flattening of effects above 35 ng/mL, in postmenopausal women but not in premenopausal.5 Unexpectedly, the meta-analysis conducted by Ordonez-Mena et al12 showed increased breast cancer risk with higher 25(OH)D concentrations. The different finding of this study from the previous other meta-analysis studies may be explained by different settings, different enrolled populations, and differences in the adjusted levels. The study by Ordonez- Mena et al12 enrolled cohort data from European population- based cohort studies, whereas the previous studies enrolled nested case-control studies conducted in the United States with different adjustments for confounders.
The inverse association between vitamin D level and breast cancer risk was also shown in pooled and review studies. Mohr et al13 reported in their pooled analysis of 11 case-control studies that individuals in the highest quintile versus the lowest quintile of 25(OH)D concentrations had a reduction in breast cancer risk, in which serum 25(OH)D level of 47 ng/mL was associated with a 50% lower risk of breast cancer. Similar inverse association was also reported by Stoll et al14 in their systematic review of 37 studies. They suggested that elevated serum 25(OH)D through the sun exposure and dietary intake more than 400 IU per day vitamin D supplementation decreased breast cancer risk and recurrence. Similar findings were also reported by Shekarriz-Foumani et al4 in their systematic review who reviewed 13 studies and found that serum 25(OH)D deficiency has been very prevalent among breast cancer neoplasms.
For breast cancer-controlled studies, case-control studies consistently find an inverse correlation between 25(OH)D and breast cancer risk.15,16 Bilinski et al15 showed that 25(OH)D concentration below 75 nmol/L at diagnosis was associated with a significantly higher risk of breast cancer. Compared with subjects with sufficient 25(OH)D concentration, the ORs of breast cancer were 2.3 (95% CI = 1.3-4.3), 2.5 (95% CI = 1.63.9), and 2.5 (95% CI = 1.6-3.8) for subjects categorized as severely deficient, deficient, or insufficient vitamin D status, respectively.15 Other studies have found similar reduction in the risk for breast cancer. Park et al16 found that serum 25(OH) D less than 20 ng/mL was associated with 27% increased risk of breast cancer. Similar results have been reported by Colagar et al,25 Bertrand et al,26 Reimers et al,27 and Kim et al.28 The prevalence of vitamin D deficiency in breast cancer population has ranged from 23% to 95.6%.4 Jamshidinaeini et al18 found that women in the fourth quartile of serum 25(OH)D level had 3 times lower risk of developing breast cancer compared with those in the first quartile. Inverse association was only seen in premenopausal women (OR = 0.25; 95% CI = 0.094-0.687). They also found that dietary intake of vitamin D was inversely associated with breast cancer risk (OR fourth quartile versus first quartile = 0.39; 95% CI = 0.196-0.784), and this inverse association remained significant after adjusting for the confounding factors.18 Similar results were reported by Shaukat et al19 who studied 42 newly diagnosed breast cancer cases and 52 controls. They found that serum vitamin D levels were significantly lower in cases (85.7%) compared with controls (55.8%). The unadjusted and adjusted ORs for breast cancer in cases and controls showed a statistically significantly increased risk of breast cancer. After adjustment for age, parity, body mass index, sun exposure, economic status, and education status, the OR (95% CI) for breast cancer risk was 7.8 (1.9930.58) for women with vitamin D concentrations less than 20 ng/mL.19 To support the robust nature of breast cancer case- control studies, Grant shows that results of 11 studies from 7 countries align in a robust power-law fit to the OR versus mean 25(OH)D concentrations. He showed that 25(OH)D concentration values are only useful for short follow-up times for breast cancer as it develops rapidly. 17
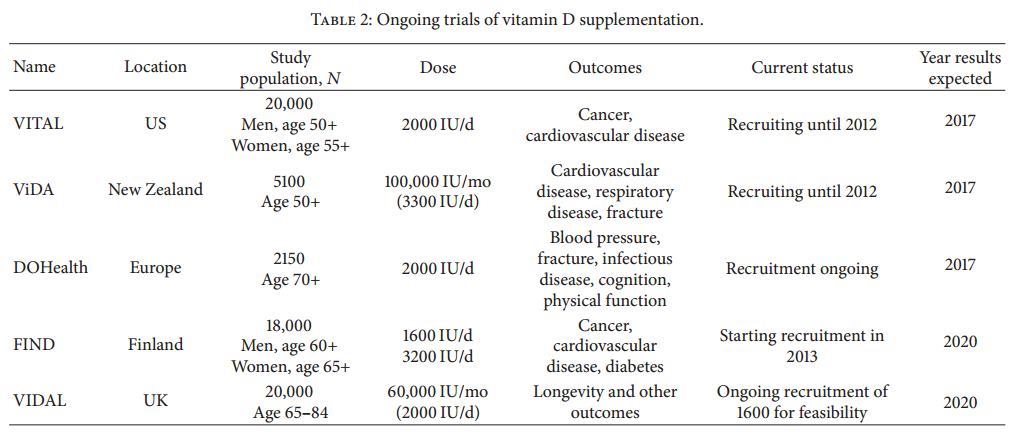
Although most case-controlled studies, meta-analysis, and pooled reviews found that 25(OH)D concentration was inversely related to breast cancer risk, only a few randomized controlled trials (RCTs) of vitamin D support this finding. Bolland et al20 in their study of the Women’s Health Initiative randomized trial showed that among 15 646 women (43%) who were not taking personal calcium or vitamin D supplements at randomization, coadministered calcium and vitamin D significantly decreased the risk of total breast and invasive breast cancers by 14% to 20%. In contrast, Neuhouser et al21 in another Women’s Health Initiative randomized trial did not find an association between vitamin D and breast cancer risk, in their multivariate-adjusted breast cancer models, and the associations were not significant (OR = 1.06; 95% CI = 0.78-1.43).
McDonnell et al22 in their pooled analysis of the randomized trial and prospective cohort study (Table 1) support this inverse association between 25(OH)D concentration and risk of breast cancer and highlighted the importance of cancer prevention by achieving 25(OH)D substantially above 20 ng/ mL. They reported that women with 25(OH)D concentration more than 20 ng/mL had 67% lower risk of any invasive cancer compared with serum 25(OH)D less than 20 ng/mL.22 Lappe et al24 found in a randomized clinical trial among healthy postmenopausal women with a mean baseline serum 25(OH)D level of 32.8 ng/mL, supplementation with vitamin D3, and calcium compared with placebo did not result in a significantly lower risk of cancer at 4 years. The reason for lack of support between 25(OH)D levels and breast cancer risk in most RCTs is the poor design of some RCTs. Most vitamin D RCTs to date have considered the vitamin D dose, rather than initial, final, or changes in serum 25(OH)D concentrations. So a recent study by Grant and Boucher23 developed a model for use in designing and analyzing vitamin D RCTs with application to cancer incidence. Model input variables are vitamin D dose, baseline and achieved 25(OH)D concentrations, known rates of cancer for the population, and numbers of participants for the treatment. This model may improve vitamin D RCT.
Vitamin D deficiency increased the risk for breast cancer among both pre- and postmenopausal women. Bidgoli et al29 have studied serum 25(OH)D levels in Iran among newly diagnosed premenopausal women with breast cancer and showed more than 50% of analyzed individuals had very severe or severe vitamin D deficiency. The 25-hydroxyvitamin D deficiency caused 7.5-fold greater risk among postmenopausal breast cancer women compared with control.28 Likewise, 25(OH)D levels more than 38.0 ng/mL and regular vitamin D supplementation were associated with lower breast cancer among postmenopausal women.30
It is very important to conduct vitamin D RCTs, and according to the model by Grant and Boucher,23 that would start the trial with a moderate bolus dose to achieve the desired 25(OH)D concentrations among both pre- and postmenopausal women, and blood spot 25(OH)D assay use in summer and winter annually to monitor seasonal and long-term changes in 25(OH)D concentration and compliance, and to allow dosage adjustment for achievement of desired vitamin D status. The results of these trials are a key prevention tool for primary prevention of cancer rather than expanding early detection or improving treatment.
Low levels of vitamin D were recorded among patients with breast cancer compared with healthy controls.31 Moreover, low vitamin D levels were common at breast cancer diagnosis and were associated with a poor prognosis; about 94% women with vitamin D level less than 20 ng/mL develop metastases and 73% die of the advanced disease.32 The 25(OH)D levels are significantly higher in patients with early-stage breast cancer compared with those with locally advanced or metastatic disease.33 The relationship between vitamin, breast cancer, and prognostic factors such as tumor stage, grade, size, lymph node involvement, and hormone receptors status is contradictory. The 25-hydroxyvitamin D level had a significant inverse association with metastatic breast cancer.34 Low vitamin D levels were associated with advanced stages of the disease, tumor size, and grade in postmenopausal patients,34 as well as in premenopausal women with triple-negative cancer.35 Insufficient and deficient 25(OH)D levels had a higher proportion of tumors with locally advanced and metastatic disease, more positive lymph node, a lower proportion of ER-positive, progesterone receptor-positive tumors, and higher Ki-67.36 Normal vitamin D patients had a higher frequency of luminal A (47.7%) and luminal B (32.2%) tumors when compared with patients with vitamin D insufficiency or deficiency.36 Similar results were reported by a South Korean study, which showed a significant association between low levels of 25(OH)D and poor outcome in breast cancer and triple-negative tumors.37 By contrast, no relationship between serum vitamin D levels and any of the tumor prognostic features was shown by the study conducted by Imtiaz et al.38 This inconsistency among different studies may be related to differences in sample sizes and limitations of demographic data related to ethnicity and lifestyle. The menopausal status may be another factor associating with vitamin D status and* VDR *polymorphism must also be considered. In addition, modifying effects of environmental factors, such as dietary factors, candidate gene variants of other genes of vitamin D pathways, such as vitamin D-binding proteins, and enzymes that involve in the activation and degradation of vitamin D, such as CYP2R1, CYP27A1, CYP27B1, and CYP24A1, must also be considered.
Vitamin D exerts its effects via* VDR , which is found in breast epithelial cells. Vitamin D receptor was first identified in a breast cancer cell line in 1979 and later identified in human breast tumor tissues.39 It has an intracellular hormone receptor that binds to 1,25(OH)2D and interacts with VDR response elements of target genes. Vitamin D regulates the transcription of more than 60 genes that are responsible for antiproliferative, prodifferentiating, antimetastatic, and proapoptotic effects on cells.8,13 Decreased serum vitamin D levels result in enriched cellular growth, neoangiogenesis, and cancer development, and VDR knockout mice showed higher rates of preneoplastic mammary lesions.40 A recent study7 suggests that a potential mechanism underlying the link between vitamin D levels and breast cancer is by regulating autophagy within both normal mammary epithelial cells and luminal breast cancer cells. This may pinpoint the role of vitamin D and its receptor *in modulating autophagy and highlight the potential of using vitamin D as a cancer-preventive agent.
The* VDR gene lies on the long arm of chromosome 12 (12q12-14), with more than 200 single-nucleotide polymorphisms verified in it.41 The most common studied allelic variants within VDR were as follows: Fokl (T/C) in exon II, BsmI (A/G) and ApaI (C/A) between exon VII and IX, TaqI (T/C) variant in exon IX,42 and poly(A).43 Reports show which of these polymorphisms associated with breast cancer are inconsistent (Table 2). Iqbal and Khan6 in their systematic metaanalysis showed that VDR gene polymorphisms, Bsm1, Apa1, poly(A), Fokl, and Apal, were associated with the breast cancer, whereas Cdx2, Bgll, and Taql polymorphisms did not show any association. In another meta-analysis conducted by Laczmanski et al44 for 125 951 persons from 135 populations, Fokl VDR polymorphism was associated with increased breast cancer risk (OR=0.96; 95% CI = 0.93-0.99. Another metaanalysis of 8 studies did not show any significant association between Fok1, Bsm1, Taq1, Apa1, VDR polymorphism, and breast cancer risk (Table 2).45 The VDR polymorphism case- control studies (Table 2) showed different associations between different VDR polymorphisms and breast cancer risk among different populations: ApaI and TaqI confer high breast cancer susceptibility among Egyptian women,46 Taq1 among Jordanian women,47 Bsma1 among Pakistani women,48 and poly(A) microsatellite among Iranian women.25 BsmI but not Fok1 was associated with the risk of breast cancer among Iranian women.49 However, Shaikh et al50 in their mini review compare the impact of VDR gene polymorphisms, Fok1, Bsm1, Taq1, Apa1, and poly(A), on the development of breast cancer and showed inconsistent results, with no conclusive statements about the significance of the VDR *genotype on breast carcinoma development (Table 2).
Conclusions
This review shows that most of the vitamin D studies support the inverse association between vitamin D level and breast cancer risk, and retrospective and prospective epidemiologic studies revealed that vitamin D deficiency is associated with increased breast cancer risk. Nonetheless, there is an urgent need for better designed and randomized clinical trials that will address the association of vitamin D level with breast cancer risk, breast cancer development, recurrence, and survival at different breast cancer stages. These trials can be developed according to the model by Grant and Boucher23 for designing and analyzing vitamin D RCT with application to cancer incidence. Input variables will be vitamin D dose, baseline and achieved 25(OH)D concentrations, known rates of cancer for the population, and numbers of participants for the treatment. These studies should be applied to different population ethnicities, for pre- and postmenopausal women, with* VDR *polymorphism screening. The lifestyle, dietary factors, and gene variants of other genes that influence vitamin D pathways, such as vitamin D-binding proteins, and the enzymes that involve in vitamin D activation, such as CYP2R1, CYP27A1, CYP27B1, and CYP24A1, should also be taken into account.
REFERENCES
Enko D, Kriegshauser G, Stolba R, Worf E, Halwachs-Baumann G. Method evaluation study of a new generation of vitamin D assays. Biochem Med (Zagreb). 2015;25:203-212.
Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin EndocrinolMetab. 2011;96:53-58.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-1930. doi:10.1210/jc.2011-0385.
Shekarriz-Foumani R, Khodaie F. The correlation of plasma 25-hydroxyvitamin D deficiency with risk of breast neoplasms: a systematic review. Iran J Cancer Prev. 2016;9:e4469. doi:10.17795/ijcp-4469.
Bauer SR, Hankinson SE, Bertone-Johnson ER, Ding EL. Plasma vitamin D levels, menopause, and risk of breast cancer: dose-response meta-analysis of prospective studies. Medicine. 2013;92:123-131. doi:10.1097/MD.0b013e3182943bc2.
Iqbal MUN, Khan TA. Association between vitamin D* receptor *(Cdx2, Fok1, Bsm1, Apa1, Bgl1, Taq1, and Poly (A)) gene polymorphism and breast cancer: a systematic review and meta-analysis. Tumour Biol. 2017;39:1010428317731280. doi:10.1177/1010428317731280.
Tavera-Mendoza LE, Westerling T, Libby E, et al. Vitamin D* receptor *regulates autophagy in the normal mammary gland and in luminal breast cancer cells. Proc Natl Acad Sci U S A. 2017;114:E2186-E2194. doi:10.1073/pnas.1615015114.
Khan MI, Bielecka ZF, Najm MZ, et al. Vitamin D* receptor *gene polymorphisms in breast and renal cancer: current state and future approaches (review). Int J Oncol. 2014;44:349-363.
Eliassen AH, Warner ET, Rosner B, et al. Plasma 25-hydroxyvitamin D and risk of breast cancer in women followed over 20 years. Cancer Res. 2016;76:5423- 5430. doi:10.1158/0008-5472.CAN-16-0353.
Uray IP, Brown PH. Chemoprevention of hormone* receptor *-negative breast cancer: new approaches needed. Recent Results Cancer Res. 2011;188:147-162. doi:10.1007/978-3-642-10858-7_13.
Chen P, Hu P, Xie D, Qin Y, Wang F, Wang H. Meta-analysis of vitamin D, calcium and the prevention of breast cancer. Breast Cancer Res Treat. 2010;121: 469-477.
Ordonez-Mena JM, Schottker B, Fedirko V, et al. Pre-diagnostic vitamin D concentrations and cancer risks in older individuals: an analysis of cohorts participating in the CHANCES consortium. Eur J Epidemiol. 2016;31:311-323. doi:10.1007/s10654-015-0040-7.
Mohr SB, Gorham ED, Alcaraz JE, et al. Serum 25-hydroxyvitamin D and prevention of breast cancer: pooled analysis. Anticancer Res. 2011;31:2939-2948.
Stoll F, Akladios CY, Mathelin C. Vitamin D and breast cancer: is there a link? Gynecol Obstet Fertil. 2013;41:242-250.
Bilinski K, Boyages J. Association between 25-hydroxyvitamin D concentration and breast cancer risk in an Australian population: an observational case-controlstudy. Breast Cancer Res Treat. 2013;137:599-607. doi: 10.1007/s 10549012-2381-1.
Park S, Lee DH, Jeon JY, et al. Serum 25-hydroxyvitamin D deficiency and increased risk of breast cancer among Korean women: a case-control study. Breast Cancer Res Treat. 2015;152:147-154. doi:10.1007/s10549-015-3433-0.
Grant WB. 25-Hydroxy vitamin D and breast cancer, colorectal cancer, and colorectal adenomas: case-control versus nested case-control studies. Anticancer Res. 2015;35:1153-1160.
Jamshidinaeini Y, Akbari ME, Abdollahi M, Ajami M. Davoodi SH. Vitamin D status and risk of breast cancer in Iranian women: a case-control study. J Am Coll Nutr. 2016;35:639-646.
Shaukat N, Jaleel F, Moosa FA, Qureshi NA. Association between vitamin D deficiency and breast cancer. Pak J Med Sci. 2017;33:645-649. doi: 10.12669/ pjms.333.11753.
Bolland MJ, Grey A, Gamble GD, Reid IR. Calcium and vitamin D supplements and health outcomes: a reanalysis of the Women’s Health Initiative (WHI) limited-access data set. Am J Clin Nutr. 2011;94:1144-1149. doi: 10.3945/ ajcn.111.015032.
Neuhouser ML, Manson JE, Millen A, et al. The influence of health and lifestyle characteristics on the relation of serum 25-hydroxyvitamin D with risk of colorectal and breast cancer in postmenopausal women. Am J Epidemiol. 2012;175:673-684. doi:10.1093/aje/kwr350.
McDonnell SL, Baggerly C, French CB, et al. Serum 25-hydroxyvitamin D concentrations >40 ng/ml are associated with >65% lower cancer risk: pooled analysis of randomized trial and prospective cohort study. PLoS ONE. 2016;11:e0152441. doi:10.1371/journal.pone.0152441.
Grant WB, Boucher BJ. Randomized controlled trials of vitamin D and cancer incidence: a modeling study. PLoS ONE. 2017;12:e0176448. doi:10.1371/jour- nal.pone.0176448.
Lappe J, Watson P, Travers-Gustafson D, et al. Effect of vitamin D and calcium supplementation on cancer incidence in older women: a randomized clinical trial. JAMA. 2017;317:1234-1243. doi:10.1001/jama.2017.2115.
Colagar AH, Firouzjah HM. Halalkhor S. Vitamin D* receptor *poly(A) microsatellite polymorphism and 25-hydroxyvitamin D serum levels: association with susceptibility to breast cancer. J Breast Cancer. 2015;18:119-125. doi:10.4048/ jbc.2015.18.2.119.
Bertrand KA, Rosner B, Eliassen AH, et al. Premenopausal plasma 25-hydroxyvitamin D, mammographic density, and risk of breast cancer. Breast Cancer Res Treat. 2015;149:479-487. doi:10.1007/s10549-014-3247-5.
Reimers LL, Crew KD, Bradshaw PT, et al. Vitamin D-related gene polymorphisms, plasma 25-hydroxyvitamin D, and breast cancer risk. Cancer Causes Control. 2015;26:187-203. doi:10.1007/s10552-014-0497-9.
Kim Y, Franke AA, Shvetsov YB, et al. Plasma 25-hydroxyvitamin D3 is associated with decreased risk of postmenopausal breast cancer in whites: a nested case-control study in the multiethnic cohort study. BMC Cancer. 2014;14:29. doi:10.1186/1471-2407-14-29.
Bidgoli SA, Azarshab H. Role of vitamin D deficiency and lack of sun exposure in the incidence of premenopausal breast cancer: a case control study in Sabzevar, Iran. Asian Pac J Cancer Prev. 2014;15:3391-3396.
O’Brien KM, Sandler DP, Taylor JA, Weinberg CR. Serum vitamin D, risk of breast cancer within five years. Environ Health Perspect. 2017;125:077004. doi:10.1289/EHP943.
Hatse S, Lambrechts D, Verstuy A, et al. Vitamin D status at breast cancer diagnosis: correlation with tumor characteristics, disease outcome, and genetic determinants of vitamin D insufficiency. Carcinogenesis. 2012;33:1319-1326. doi:10.1093/carcin/bgs187.
Imtiaz S, Siddiqui N, Raza SA, Loya A, Muhammad A. Vitamin D deficiency in newly diagnosed breast cancer patients. Indian J Endocrinol Metab. 2012;16:409- 413. doi:10.4103/2230-8210.95684.
Palmieri C, MacGregor T, Girgis S, Vigushin D. Serum 25-hydroxyvitamin D levels in early and advanced breast cancer. J Clin Pathol. 2006;59:1334-1336. doi:10.1136/jcp.2006.042747.
Janbabai G, Shekarriz R, Hassanzadeh H, Aarabi M, Borhani SS. A survey on the relationship between serum 25-hydroxy vitamin D level and tumor characteristics in patients with breast cancer. Int J Hematol Oncol Stem Cell Res. 2016;10:30-36.
Yao S, Kwan ML, Ergas IJ, et al. Association of serum level of vitamin D at diagnosis with breast cancer survival: a case-cohort analysis in the pathways study. JAMA Oncol. 2017;3:351-357. doi:10.1001/jamaoncol.2016.4188.
de Sousa Almeida-Filho B, De Luca Vespoli H, Pessoa EC, Machado M, Nahas-Neto J, Nahas EAP. Vitamin D deficiency is associated with poor breast cancer prognostic features in postmenopausal women. J Steroid Biochem Mol Biol. 2017;174:284-289. doi:10.1016/j.jsbmb.2017.10.009.
Kim HJ, Lee YM, Ko BS, et al. Vitamin D deficiency is correlated with poor outcomes in patients with luminal-type breast cancer. Ann Surg Oncol. 2011;18:1830-1836. doi:10.1245/s10434-010-1465-6.
Imtiaz S, Siddiqui N. Vitamin-D status at breast cancer diagnosis: correlation with social and environmental factors and dietary intake. J Ayub Med Coll Abbot- tabad. 2014;26:186-190.
Buras RR, Schumaker LM, Davoodi F, et al. Vitamin-D* receptor *s in breast-cancer cells. Breast Cancer Res Tr. 1994;31:191-202.
Matthews D, LaPorta E, Zinser GM, Narvaez CJ, Welsh J. Genomic vitamin D signaling in breast cancer: insights from animal models and human cells. J Steroid Biochem Mol Biol. 2010;121:362-367. doi:10.1016/j.jsbmb.2010.03.061.
Fuhrman BJ, Freedman DM, Bhatti P, et al. Sunlight, polymorphisms of vitamin D-related genes and risk of breast cancer. Anticancer Res. 2013;33: 543-551.
Slatter ML, Yakumo K, Hoffman M, Neuhausen S. Variants of the* VDR *gene and risk of colon cancer (United States). Cancer Causes Control. 2001;12: 359-364.
Alimirah F, Peng X, Murillo G, Mehta RG. Functional significance of vitamin D* receptor *FokI polymorphism in human breast cancer cells. PLoS ONE. 2011;6:e16024. doi:10.1371/journal.pone.0016024.
Laczmanski L, Lwow F, Osina A, Kepska M, Laczmanska I, Witkiewicz W. Association of the vitamin D* receptor *FokI gene polymorphism with sex- and non-sex-associated cancers: a meta-analysis. Tumour Biol. 2017;39:1010428 317727164. doi:10.1177/1010428317727164.
Lu D, Jing L, Zhang S. Vitamin D* receptor *polymorphism and breast cancer risk: a meta-analysis. Medicine. 2016;95:e3535. doi:10.1097/MD.000000000 0003535.
El-Shorbagy HM, Mahmoud NH, Sabet S. Association of vitamin D* receptor *gene polymorphisms with breast cancer risk in an Egyptian population. Tumour Biol. 2017;39:1010428317727738. doi:10.1177/1010428317727738.
Atoum MF, Al-Khatib YM. Association between serum 25-hydroxy vitamin D concentration and TaqI vitamin D* receptor *gene polymorphism among Jordanian females with breast cancer. Chinese Med J. 2017;130:1074-1078. doi:10.4103/ 0366-6999.204933.
Rashid MU, Muzaffar M, Khan FA, et al. Association between the Bsml polymorphism in the vitamin D* receptor *gene and breast cancer risk: results from a Pakistani case-control study. PLoS ONE. 2015;10:e0141562. doi:10.1371/jour-nal.pone.0141562
Shahabi A, Alipour M, Safiri H, et al. Vitamin D* receptor *gene polymorphism: association with susceptibility to early-onset breast cancer in Iranian, BRCA1/2- mutation carrier and non-carrier patients. Pathol Oncol Res. 2017;174:284-289. doi:10.1007/s12253-017-0281-8.
Shaikh F, Baig S, Jamal Q. Do** VDR__ gene polymorphisms contribute to breast cancer? Asian Pac J Cancer Prev. 2016;17:479-483.