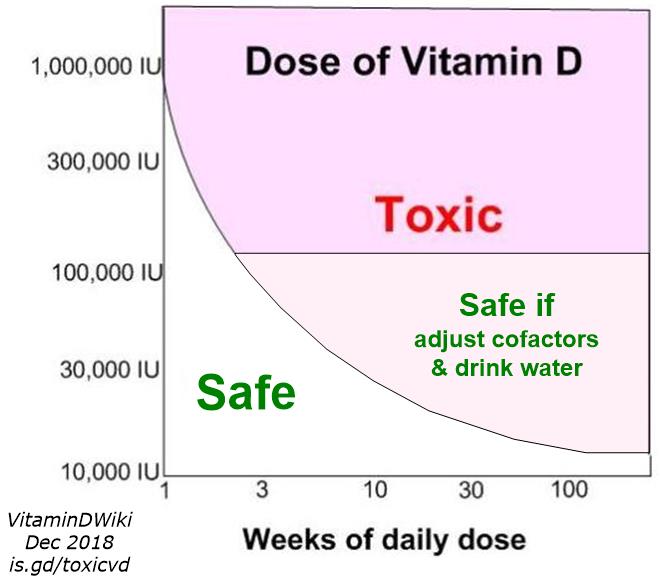
10,000 IU vitamin D daily is safe, toxicity start at 150 ng (for monotherapy)
Anti-Cancer Agents in Medicinal Chemistry Volume 13 Issue 1 pp.4-10 (7)
Authors: Armin Zittermann, Sylvana Prokop, Jan F. Gummert, Jochen Borgermann
 1. Summary of points of this paper by Vitamin D Council Dec 2012
1. Data on skin synthesis of vitamin D indicate oral intake of 10,000 IU/day is safe.
1. The half-life of 25(OH)D3 is about 3 weeks. That is, it takes about 3 weeks for the body to metabolize one-half of a dose of vitamin D.
* However, this depends on initial levels, the lower the initial level the longer the half-life.
1. Vitamin D intoxication is rare, while vitamin D deficiency is widespread and a “re-emerging global health problem.”
1. Excessive vitamin D intake leads to low blood phosphate levels.
1. Vitamin D toxicity is probably caused by the effects of elevated 25(OH)D itself, not by elevated 1,25(OH)D levels.
1. Professor Hector DeLuca of the University of Wisconsin, recently concluded that high blood calcium might occur in some people after prolonged daily doses of 25,000 IU/day.
1. 10,000 IU/day for six months in young men led to mean 25(OH)D levels of 90 ng/ml.
1. 5,000 IU/day for six months in young men led to mean 25(OH)D levels of 53 ng/ml.
1. Dr John Hathcock’s analysis of 20 publications showed no ill effects of using 10,000 IU/day.
1. Most reports indicate the toxicity threshold is somewhere between 10,000 and 40,000 IU/day.
1. High intermittent doses of vitamin D, such as monthly doses, should be avoided.
1. A high initial serum 25(OH)D level somehow allows the body to rid itself of most of an additional dose of vitamin D.
1. When 25(OH)D3 is used as a drug, it is five times more potent than vitamin D3. It used to be available in the USA as Calderol and Delakmin.
1. According to the Institute of Medicine’s Food and Nutrition Board, the upper safe blood level for 25(OH)D is 50 ng/ml.
* However, according to Dr Zimmermann, this recommendation “is not well documented.” Certainly, much higher levels are seen with sun exposure alone.
1. How much vitamin D one needs depends on body weight, with 20-40 IU/kg/day needed to increase blood levels by 20 ng/ml.
1. Summary of points of this paper by Vitamin D Council Dec 2012
1. Data on skin synthesis of vitamin D indicate oral intake of 10,000 IU/day is safe.
1. The half-life of 25(OH)D3 is about 3 weeks. That is, it takes about 3 weeks for the body to metabolize one-half of a dose of vitamin D.
* However, this depends on initial levels, the lower the initial level the longer the half-life.
1. Vitamin D intoxication is rare, while vitamin D deficiency is widespread and a “re-emerging global health problem.”
1. Excessive vitamin D intake leads to low blood phosphate levels.
1. Vitamin D toxicity is probably caused by the effects of elevated 25(OH)D itself, not by elevated 1,25(OH)D levels.
1. Professor Hector DeLuca of the University of Wisconsin, recently concluded that high blood calcium might occur in some people after prolonged daily doses of 25,000 IU/day.
1. 10,000 IU/day for six months in young men led to mean 25(OH)D levels of 90 ng/ml.
1. 5,000 IU/day for six months in young men led to mean 25(OH)D levels of 53 ng/ml.
1. Dr John Hathcock’s analysis of 20 publications showed no ill effects of using 10,000 IU/day.
1. Most reports indicate the toxicity threshold is somewhere between 10,000 and 40,000 IU/day.
1. High intermittent doses of vitamin D, such as monthly doses, should be avoided.
1. A high initial serum 25(OH)D level somehow allows the body to rid itself of most of an additional dose of vitamin D.
1. When 25(OH)D3 is used as a drug, it is five times more potent than vitamin D3. It used to be available in the USA as Calderol and Delakmin.
1. According to the Institute of Medicine’s Food and Nutrition Board, the upper safe blood level for 25(OH)D is 50 ng/ml.
* However, according to Dr Zimmermann, this recommendation “is not well documented.” Certainly, much higher levels are seen with sun exposure alone.
1. How much vitamin D one needs depends on body weight, with 20-40 IU/kg/day needed to increase blood levels by 20 ng/ml.
Vitamin D deficiency is a re-emerging global health problem, which is primarily due to inadequate vitamin D synthesis in the skin. Supplement use is an effective measure to improve vitamin D status. However, some safety issues have to be considered, which are highlighted in this review article: The concept of vitamin D safety consists of two models, the safe tolerable upper intake level (UL) method, and the idea of adequate circulating 25-hydroxyvitamin D (25[OH]D) levels. Oral vitamin D intakes up to 250 μg/d have not been associated with harm. Hypercalcemia, the hallmark of vitamin D intoxication, may only occur if circulating 25(OH)D levels are consistently above 375-500 nmol/l. However, some observational studies indicate that already circulating 25(OH)D levels > 125 nmol/l are related to an increased morbidity and mortality risk. Therefore, the Institute of Medicine has set the UL for adults at 100 μg/d, and the adequate circulating 25(OH)D level at 50 to 125 nmol/l. In clinical practice, oral vitamin D dosing has to consider that the increment in circulating 25(OH)D depends on baseline 25(OH)D levels and the person's body weight. It is reasonable to assess 25(OH)D before and 3-6 months after initiation of oral vitamin D administration and to adjust the dose, if necessary. In future, two issues have to be clarified: First, would it be more appropriate to define instead of a fixed UL a variable UL, based on the individual's body weight? Second, what are the underlying mechanisms, if any, for potentially harmful vitamin D effects at circulating 25(OH)D levels between 125 and 375 nmol/l.
Affiliation: Clinic for Thoracic and Cardiovascular Surgery, Heart and Diabetes Center North Rhine-Westphalia, Ruhr University Bochum, Georgstraße 11, 32545 Bad Oeynhausen, Germany.
PDF is attached at the bottom of this page
INTRODUCTION
Vitamin D is unique among vitamins in that humans can produce it themselves in their skin provided they have sufficient exposure to ultraviolet (UV) B radiation (290-315 nm). Skin synthesis of vitamin D is very effective. It is assumed that already 10 to 15 minutes of summer sun exposure are sufficient to produce adequate amounts of vitamin D. Daily full-body exposure to solar UVB-radiation can be equivalent to an oral vitamin D intake of 250 ug (10,000 international units (IU), to convert ug into IU multiply by 40) [1] and probably even more [2]. It is also noteworthy, that there are no reports of vitamin D intoxications after intensive solar UVB irradiation [3]. This is due to the fact that daily skin synthesis of vitamin D reaches a plateau when 15% of the vitamin D precursor 7-dehydrocholesterol is converted into vitamin D. Thereafter, vitamin D-inactive substances such as lumisterol and tachysterol are produced [4]. Data on skin synthesis of vitamin D are thus a first indication that in apparently healthy free-living individuals a daily amount of up to 250 ug (10,000 IU) is safe.
For a better understanding of toxic vitamin D effects, the following paragraph will briefly highlight some aspects of vitamin D metabolism: Usually, skin synthesis contributes to approximately 80-90% to human vitamin D status. Dietary intake is a second source of vitamin D. However, only a few marine foods such as eel, herring and salmon are vitamin D-rich foods, whereas the vitamin D content of the vast majority of other foods is very small or even zero. Therefore, in the absence of effective food fortification programs, dietary vitamin D intake does not exceed 3-5 ug per day in most individuals [5]. This explains why dietary vitamin D intake usually contributes only 10-20% to human vitamin D status. In some populations with a traditionally high intake of specific, vitamin D-rich marine foods, however, daily vitamin D intakes of 54-62 ug (2,160-2,480 IU) have been reported [6].
Once in the circulation, vitamin D is converted by a hepatic hydroxylase into 25-hyroxyvitamin D (25[OH]D). The circulating 25(OH)D level is the best indicator of human vitamin D status. This level reflects both, skin synthesis of vitamin D and dietary vitamin D intake. The half-life of 25(OH)D in the circulation is approximately 3 weeks. As needed, 25(OH)D is converted in the kidney to its active hormonal form 1,25-dihydroxyvitamin D (1,25[OH]2D) in a process which is usually tightly controlled by parathyroid hormone (PTH) and the phosphaturic hormone fibroblast growth factor (FGF)-23 [7]. A high percentage of all vitamin D metabolites circulating in the blood are bound to a vitamin D specific transport protein, which is named vitamin D binding protein (DBP). The total binding capacity of DBP for vitamin D metabolites is approximately 4700 nmol/l (to convert nmol 25(OH)D per liter into ng 25(OH)D per millilitre divide by 2.496) [8]. Only a small portion of vitamin D metabolites circulate in the blood in a "free" biologically active form. Cellular vitamin D actions are mediated by a membrane-bound and a cytosolic vitamin D receptor (VDR). The VDR is nearly ubiquitously expressed, and almost all cells respond to vitamin D exposure. Whereas classical vitamin D actions are related to an improvement in intestinal calcium and phosphate absorption, nonclassical actions include important functions in the regulation of cell metabolism, differentiation, and communication.
In contrast to renal 1 a-hydroxylation, hepatic 25-hydroxylation of vitamin D is not homeostatically regulated. Notably, intestinal absorption of orally ingested vitamin D is quantitative, even after ingestion of high doses. Therefore, very high circulating 25(OH)D levels can occur after excessive oral vitamin D intake.
It is however noteworthy that vitamin D intoxication is rarely seen in the general population. In contrast, vitamin D deficiency is widespread and a re-emerging global health problem [9]. The main factors being responsible for lower 25(OH)D levels are older age, female sex, higher geographic latitude, winter season, darker skin pigmentation, less sunlight exposure, avoidance of vitamin D-rich foods and absence of effective vitamin D fortification. Therefore, effective measures to improve vitamin D status are needed. Although exposure to artificial UVB-radiation, e.g. in institutionalized individuals is possible and also effective, this measure is generally time-consuming for all persons involved and can simultaneously only be applied to a small group of individuals. Vitamin D supplements bear the opportunity to improve vitamin D status orally. This measure is inexpensive, effective, and easy to handle. However, huge amounts of vitamin D can theoretically be administered orally. Therefore, some safety issues have to be considered, which are highlighted in this article.
CAUSES AND SYMPTOMS OF VITAMIN D INTOXICATION
Cases of vitamin D intoxication have been described (i) in patients with established osteoporosis after prescription of excessive therapeutic vitamin D doses [10,11], (ii) in individuals who took over-the-counter supplements that accidently contained vitamin D amounts which were several hundred-fold higher than declared [12,13], and (iii) in persons who drank milk from a home-delivery dairy, which was accidently overfortificated with vitamin D [14,15]. Vitamin D intoxications have also been reported in British infants during the late 1940s and early 1950s after heavy enrichment of dried milk powder together with vitamin D-enriched cereals and in addition to the recommendation of a daily vitamin D supplement of 17.5-20.0 ng (700-800 IU) [16]. Moreover, the oral bolus administration in the former German Democratic Republic against rickets with intermittent doses of 15 mg vitamin D2 (600,000 IU) was associated with symptoms of vitamin D intoxications [17,18].
The hallmark of vitamin D intoxication is hypercalcemia, which is due to intestinal calcium hyperabsorption and above all to calcium resorption from bone. Excess vitamin D does also lead to hyperphoshatemia. Hypercalcemia and hyperphosphatemia cause mineralization of various soft tissues including kidneys, heart, aorta, other blood vessels, and cutaneous tissue [19]. Hypercalciuria may occur in the absence of hypercalcemia and is related to either hyperabsorption of calcium in the gut or a renal leak whereby calcium excretion is enhanced. Both etiologies can lead to nephrocalcinosis [20]. Vitamin D intoxicated patients suffer from headache, nausea, vomiting, diarrhea, anorexia, weight loss, polyuria and polydypsia. Excess vitamin D intake has also been made responsible for several documented deaths [19]. Vitamin D intoxication has been widely used as an experimental model for vascular disease [21].
MECHANISMS OF VITAMIN D INTOXICATION
Three major theories about the mechanism of vitamin D intoxication have been proposed [22]. All involve increased blood concentrations of a vitamin D metabolite reaching the VDR of a target cell. Possible mechanisms of vitamin D intoxication after excessive oral vitamin D intake include (i) the rise of circulating 1,25(OH)2D concentrations into the toxic range, (ii) the rise of circulating 25(OH)D to umol/l concentrations and (iii) the rise of blood concentrations of many vitamin D metabolites thereby causing release of "free" 1,25(OH)2D, which enters its target cells
Studies in genetically modified mice, such as FGF23-/- and Klotho-/- mice that exhibit altered mineral homeostasis due to high circulating 1,25(OH)2D levels showed features of premature aging that include retarded growth, osteoporosis, atherosclerosis, ectopic calcification, immunological deficiency, skin and general organ atrophy, hypogonadism and short lifespan [23]. However, evidence that excess circulating 1,25(OH)2D plays a major role in vitamin D intoxication in humans is limited to specific conditions. In most cases, where toxicity due to excessive vitamin D intake is observed, it is rarely accompanied by elevated circulating 1,25(OH)2D levels [22]. This is understandable, because circulating 1,25(OH)2D is usually tightly regulated by serum levels of PTH and FGF-23, two hormones that respond to variations in serum calcium and phosphate. In the granulomatous condition sarcoidosis, however, consistently elevated circulating 1,25(OH)2D have been described [24]. This is due to overexpression of unregulated extrarenal 1 ahydroxylase gene expression (CYP27B1) in the face of normal circulating 25(OH)D. In clinical practise, there is also a widespread use of 1,25(OH)2D or other active forms of vitamin D to treat secondary hyperparathyroidism in chronic kidney disease. Occasionally, symptoms such as hypercalcemia, hyperphoshaturia and soft tissue calcification occur, which are most certainly the result of overexposure of target cells to these physiologically active vitamin D substances [22]. However, one should clearly distinguish between the oral intake of these substances and native vitamin D.
In many cases of excess intake of native vitamin D circulating 25(OH)D levels rises to 1250 nmol/l or above. Under these conditions, circulating 1,25(OH)2D falls to almost undetectable levels [25]. This is understandable because the production of 1,25(OH)2D is suppressed by hypercalcemia and hyper-phosphatemia and the absence of PTH. 25(OH)D can, at high concentrations, become transcriptionally active, leading to excessive bone resorption and intestinal calcium and phosphate hyperabsorption. Notably, excess vitamin D intake is equally hypercalcemic in 1 a-hydroxylase-deficient mice. This clearly indicates that 1,25(OH)2D is not the toxic agent in case of excessive oral vitamin D intake and that 25(OH)D itself is probably toxicant [8].
Toxic vitamin D effects may already occur if circulating 25(OH)D concentrations are consistently above 375-500 nmol/l [22]. At these concentrations, circulating 1,25(OH)2D is still measurable. Note that 1,25(OH)2D has a relatively low affinity for DBP in plasma. In case of vitamin D intoxication, overloading by various vitamin D metabolites significantly comprises the capacity of DBP [22]. Consequently, the free concentration of circulating 1,25(OH)2D can increase significantly. This assumption is supported by findings of elevated free 1,25(OH)2D levels in a family accidentally intoxicated with vitamin D [22]. Since 1,25(OH)2D has a high affinity for the VDR in its target cells, 1,25(OH)2D is transcriptionally very active and may thus, at high cellular levels, lead to toxic vitamin D effects.
Taken together, available data indicate that all three mechanisms discussed above may exist in parallel and may contribute to toxic vitamin D effects. However, the most important mechanism is probably the toxic effect of 25(OH)D itself at supraphysiological concentrations in the circulation.
CONCEPTS OF VITAMIN D SAFETY
Vitamin D safety consists of two concepts: One idea of risk assessment of vitamin D is based on the safe tolerable upper intake level (UL) method (Fig. 1). The other model is based on the measurement of circulating 25(OH)D levels (Fig. 2). Both concepts can complete each other. The UL method involves three basic, standardized steps: hazard identification, dose-response evaluation, and derivation of the UL [26]. Hazard identification includes the collection, organization, and evaluation of all information pertaining to the adverse effects of vitamin D. This also includes identification of distinct and highly sensitive subpopulations. Animal studies can be neglected, since there is sufficient evidence from healthy adults for establishing a safe upper limit for oral intake [26].
Dose-response evaluation includes the characterization of the dose-response between vitamin D intake and adverse effects. Hypercalcemia is the classic criterion for assessing vitamin D excess. Theoretically, a no observed adverse effect level (NOAEL) and a lowest observed adverse effect level (LOAL) should be established. Plum & DeLuca [25] concluded that, overall, the toxicity of hypercalcemia becomes evident at vitamin D intakes above 625 ng/d (25,000 IU). Hathcock et al. [26], following an analysis of more than 20 publications, concluded that there was no association between harm and intakes of 250 ug/d (10,000 IU). Vitamin D intake (ug/d)
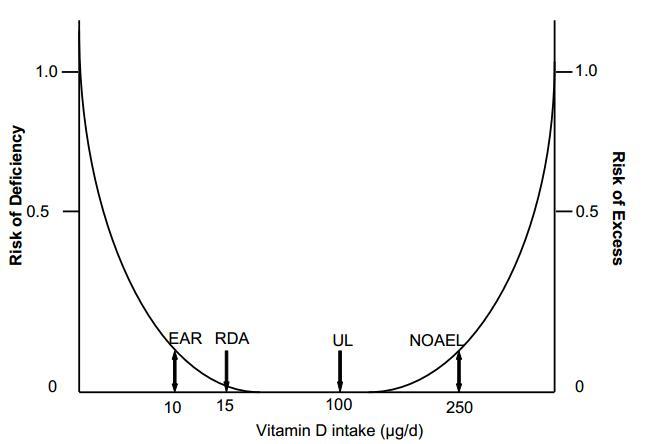
Fig. (1). Safety range of oral vitamin D intake in adults [ref. 20]. Abbreviation: EAR, estimated average requirement (is estimated to meet the requirement of 50% of healthy adults in North America); RDA, recommended dietary allowance (should meet the requirement of nearly all (97-98%) healthy adults in North America; UL, tolerable upper intake level (is the highest level of daily intake that is likely to pose no risk of adverse health effects in almost all individuals; NOAEL, no observed adverse effect level.
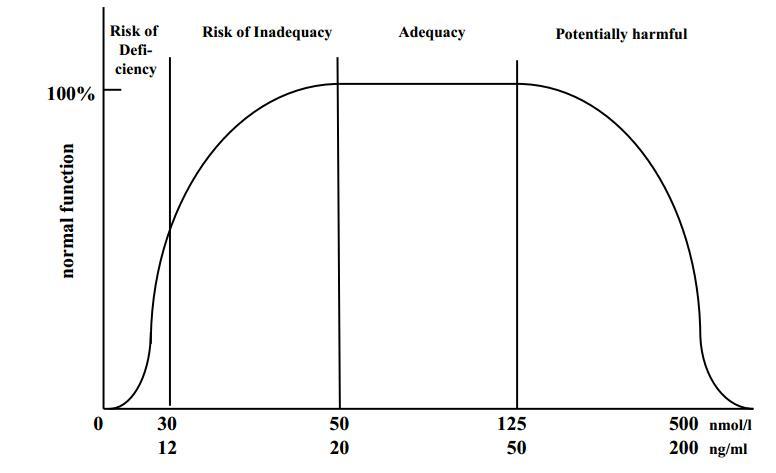
Fig. (2). Stages of vitamin D status according to circulating 25-hydroxyvitamin D level [ref. 20].
This observation is in line with the fact that exposure of skin to UV B radiation can safely provide an adult with vitamin D in an amount equivalent to an oral dose of 250 ug/d(10,000 IU). Consequently, the NOAEL can be set at 250 ug/d(10,000 IU). Most reports suggest that the toxicity threshold is between 250 ug/d(10,000 IU) and 1000 |ig (40,000 IU) of vitamin D per day [26]. It has been assumed that individuals with certain conditions, notably sarcoidosis, tuberculosis, and those treated with thiazide diuretics are extremely sensitive to excessive vitamin D. However, available data does not cast doubt on the chosen NOAEL of 250 |ig/d, (10,000 IU) even in these groups of patients [26]. It is also noteworthy that due to insufficient data, at present it is not possible to determine a LOAEL. Before an UL can be determined, uncertainties should be estimated and an uncertainty factor (UF) should be established. The larger the uncertainty, the larger the UF and the smaller the UL. Hathcock et al. [26] have proposed that there is enough evidence for the confident application of a UF of 1.0. According to this suggestion, the UL would be 250 ug/d (10,000 IU).
The circulating 25(OH)D concentration is accepted as the most appropriate indicator of vitamin D status. Selection of a NOAEL for vitamin D is aided by consideration of how circulating 25(OH)D levels relate to toxicity. Heaney et al. [27] have shown that at an intake of 250 |ig vitamin D3/day (10,000 IU), mean circulating 25(OH)D levels of 220 nmol/l are achieved, which are not associated with a change in serum calcium. Heaney's group [28] has also demonstrated that calcium absorptive input from the gut is maximized at a circulating 25(OH)D concentration of 80 nmol/l and does not rise as 25(OH)D continues to increase to at least 200 nmol/l. Based on these studies, Hathcock et al. [26] have selected a 25(OH)D level of 220 nmol/l as the healthy adult NOAEL. It is however noteworthy that the IOM has recently stated that already circulating 25(OH)D levels above 125 nmol/l should raise concerns among clinicians about potential adverse effects [29]. This statement is based on several observational findings indicating that values above this level are associated with an elevated risk of all-cause mortality and specific types of cancer [20]. In addition, there is also evidence for a U-shaped association of circulating 25(OH)D levels with allergy risk, indicating a high risk at both circulating 25(OH)D levels below 25 nmol/l and above 135 nmol/ [30]. However, it is noteworthy that these observational data do not reflect causality. High 25(OH)D levels may sometimes occur as a result of low 1,25(OH)2D levels, probably indicating deficient vitamin D actions at the cellular level [31]. In a randomized controlled trial [32], an oral bolus of 12,500 ng (500,000 IU) each autumn to winter for 3 to 5 years resulted in an increased risk of falls and fractures among older community-dwelling women. The risk was especially elevated in the first 3 months following dosing and not in the remaining 9 months of the year. One month after dosing, mean circulating 25(OH)D levels of 125 nmol/l were observed. However, if the half-life of 25(OH)D in the circulation is considered, it can reliable be assumed that 25(OH)D levels were considerably higher immediately after dosing. In a more recent study [33], a single oral bolus of 15,000 ng (600,000 IU) resulted in an acute rise of circulating 25(OH)D levels up to 168 nmol/l which was paralleled by an increase in some biochemical markers of bone resorption, indicating that intermittent high doses of vitamin D should be used with caution. Nevertheless, it is also noteworthy that oral vitamin D administration of 2,500 |ig (100,000) every four months over 5 years was safe [34].
Based on the aforementioned associations of circulating 25(OH)D levels with potentially harmful effects, the IOM followed an approach that should maximize public health protection with respect to adverse vitamin D effects. The observation that 250 |ig (10,000 IU) of vitamin D per day was not associated with classic toxicity served as the starting point for adults. In contrast to Hathcock et al. [26]; however, the IOM corrected this value for uncertainty by taking into consideration the aforementioned data on clinical outcomes, which appeared to be present at intakes lower than those associated with classic toxicity and at serum 25(OH)D concentrations previously considered to be at the high end of physiological values. Possible ethnic/racial differences were taken into account as well. Therefore, the IOM has set the upper limit of the adequate range of circulating 25(OH)D at 125 nmol/l (Fig. 2) and the UL at 100 ng/d (4,000 IU) for adults. The UL values for all age groups are presented in Table 1.
Interestingly, the IOM statement is in line with earlier suggestions that chronic exposure to solar UVB-radiation in outdoor workers produce circulating 25(OH)D levels of 122 nmol/l, which are equivalent to an oral intake of approximately 100 ng/d (4,000 IU) [26]. However, it is also noteworthy that under sun-rich living conditions mean circulating 25(OH)D levels of up to 135-163 nmol/l have been reported [35]. Since skin synthesis of vitamin D does obviously not lead to intoxication, the IOM's upper limit of the adequate range of circulating 25(OH)D seems to be very conservative.
Table 2 presents results of several recently published intervention studies with oral vitamin D doses of around 100 ng/d (4,000 IU). Data demonstrate that this dose is safe and results in mean circulating 25(OH)D levels of 75 to 160 nmol/l.
INCREMENT IN CIRCULATING 25-HYDROXYVITAMIN D ACCORDING TO ORAL VITAMIN D DOSE
As a rule of thumb, the incremental consumption of 1ug (40 IU) of vitamin D3 raises circulating 25(OH)D by 1 nmol/l [8]. This means that a person with a baseline 25(OH)D level of 25 nmol/l has to take 50 |ig vitamin D3 (2,000 IU) daily to achieve a 25(OH)D level of 75 nmol/l, a value which is considered as lower target value by many vitamin D researchers [41-43]. However, this is only a rough estimation. The increment in circulating 25(OH)D depends on various factors including the person's body weight, the initial 25(OH)D level, the administered dose and the type of oral vitamin D.
After oral vitamin D intake, the increment in 25(OH)D is remarkably similar in different age groups if the oral vitamin D3 dose is expressed per kilogram body weight. In infants, children and adults [27,38,44-46] the respective dose of vitamin D3, which results on average in an increase in circulating 25(OH)D of 50 nmol/l is in the magnitude of 0.5 |ig (20 IU) to 1.0 |ig (40 IU) per kg body weight per day (20 IU to 40 IU). This also implies that compared with lean individuals overweight and obese individuals need considerably higher daily amounts of vitamin D to achieve a similar circulating 25(OH)D level.
Aloia et al. [47] have summarized from the available literature the dose-response relationship on the increment in circulating 25(OH)D according to the administered dose. At low doses, e.g. 5 (200 IU) or 10 |ig (400 IU), an increment in 25(OH)D of up to 4 nmol/l per microgram oral vitamin D3 can be observed. At high doses, e.g. 50 |ig (2,000 IU) or 100 |ig (4,000 IU), the increment in 25(OH)D is only 0.5 to 1.0 nmol/l. Up to a dose of 35 ug/d(1,400 IU), there is a sharp nonlinear decline of the impact of dose on slope. Above this daily intake level, the serum 25(OH)D response is proportional to the dose. In total, the rate of decline per ug for doses less than 35|ig (1,400 IU) is -0.085; for doses more than 35 Hg (1,400 IU), the rate of decline is only -0.0003.
Table 1. Vitamin D Dietary Reference Intake by Life Stage [ref. 20]
Abbreviations: AI, adequate intake, EAR, estimated average requirement; RDA, recommended dietary allowance, UL, tolerable upper intake level.
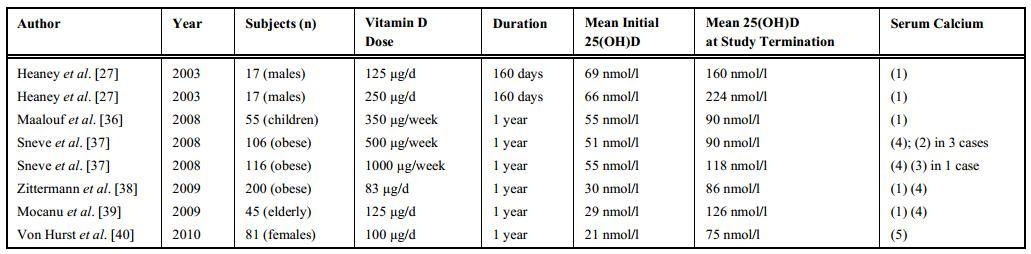
Table 2. Effects of High Dose Oral Vitamin D Intake on Circulating 25-hydroxyvitamin D and Serum Calcium Concentrations
(1) no case of hypercalcemia; (2) transient hypercalcemia; (3) Hypercalcemia, (4) unchanged serum calcium; (5) no data available.
Lips et al. [48], in a study in postmenopausal women, have demonstrated that an oral vitamin D3 intake of 10 |ig (400 IU) to 15 |ig (600 IU) daily results in a variable increment in circulating 25(OH)D, depending on initial 25(OH)D levels. At initial levels of < 25 nmol/l, 25 to 50 nmol/l and > 50 nmol/l, the increment was on average 58.4 nmol/l, 39.4 nmol/ and 13.5 nmol/l, respectively. Data indicate that at high initial 25(OH)D levels vitamin D is not quantitatively converted into 25(OH)D. A significant portion of vitamin D is obviously metabolized otherwise and does not reach the circulation.
For the improvement of circulating 25(OH)D levels, different types of vitamin D such as vitamin D2, vitamin D3 and also 25(OH)D3 are available. However, there is accumulating evidence for a considerably lower efficacy at raising circulating 25(OH)D by vitamin D2 compared with vitamin D3, diminished binding of vitamin D2 metabolites to vitamin D binding protein in plasma, and a nonphysiologic metabolism and shorter shelf life of vitamin D2 [49]. Since vitamin D3 is the physiologic form that is produced in human skin following UVB radiation, vitamin D3 supplements should be preferred. It is also noteworthy that oral 25(OH)D3 is much more effective in increasing circulating 25(OH)D compared with oral vitamin D3. Per microgram oral 25(OH)D3, a mean increment in circulating 25(OH)D of 4 nmol/l has been reported compared with 1 nmol/l per microgram oral vitamin D3 [50]. In a recent study [51], the increment in circulating 25(OH)D per microgram oral 25(OH)D3 was on average 4.8 nmol/l higher compared with the increment per microgram oral vitamin D3.
It has also to be taken into account that vitamin D is a fat soluble substance. Consequently, bioavailability may be considerably reduced if vitamin D is ingested in the fasting state. In other words, vitamin D should be administered in the non-fasting state, accompanied by a fat-containing meal.
It has been demonstrated that at the population level, a mean daily vitamin D intake of approximately 100 ug (4,000 IU) is necessary to achieve a circulating 25(OH)D level of 75 nmol/l in almost all individuals of a group whose initial 25(OH)D were on average 30 nmol/l [47]. Consequently, some vitamin D-deficient patients need more than the amount of 100 |ig daily, which the IOM has set as the UL, to achieve a circulating 25(OH)D level of 75 to 100 nmol/l. It is noteworthy that in the clinical setting even higher doses than the UL value may be administered if this is necessary and a close-meshed measurement of safety parameters such as circulating 25(OH)D, serum calcium and urinary calcium is guaranteed.
Taken all the aforementioned aspects into account, it makes sense first to measure baseline 25(OH)D levels in an individual, then to determine the daily required oral vitamin D dose (according to initial 25(OH)D level and the individual's body weight) and to reassess circulating 25(OH)D levels approximately 3-6 months later in order to adjust the oral dose, if necessary. It has been shown that the increase in circulating 25(OH)D is similar when oral vitamin D is given daily, weekly or monthly, provided that the total amount of orally ingested vitamin D is identical [52]. It is also of importance that there is no evidence for a reduction in intestinal vitamin D absorption or hepatic conversion of vitamin D into 25(OH)D with advancing age.
Vitamin D deficiency is very common [9]. Therefore, a practical vitamin D3 loading dose regimen has also been developed [53]. The loading dose required to reach the circulating 25(OH)D target level of 75 nmol/l can be calculated as follows: dose (|ig) = (75 - circulating 25[OH]D) x body weight
CONCLUSIONS
The concept of vitamin D safety consists of a UL and an adequate circulating 25(OH)D level. In adults, one microgram of oral vitamin D increases circulating 25(OH)D levels on average by 1nmol/l. Since the effect seems to be more pronounced at low initial 25(OH)D levels compared to higher 25(OH)D levels, a daily dose of 20 ug (800 IU) to 50 ug (2,000 IU) vitamin D is adequate to prevent deficient 25(OH)D levels (<30 nmol/l) in almost all individuals, even if cutaneous vitamin D synthesis is negligible. The IOM considers an oral daily intake of 100 ug (4,000 IU) as UL for all adults. However, available data indicate that it would be more appropriate to adjust oral daily vitamin D intake according to body weight. Therefore, it may sometimes be that even higher oral doses than the UL may be given to increase circulating 25(OH)D levels into the adequate range, e.g. to 75 - 100 nmol/l, a target range which has recently been associated with the lowest mortality risk in the general adult population [43]. In clinical practise, the oral daily vitamin D dose should be determined and adjusted, if necessary, by measuring circulating 25(OH)D before and 3-6 months after dosing.
According to the IOM, the upper safe level of circulating 25(OH)D is 125 nmol/l. However, this upper cut-off value is not well documented and primarily relies on observational studies. According to the available literature on the hallmark of vitamin D safety, which is serum calcium, even higher 25(OH)D levels than 125 nmol/l do not cause harm. Additional studies are therefore still needed to determine the upper safe level of circulating 25(OH)D more appropriate.
REFERENCES
[I] Engelsen, O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients, 2010, 2(5), 482-495.
[2] Holick, M.F. Vitamin D: the underappreciated D-lightful hormone that is important for skeletal and cellular health. Curr. Opin. Endocrinol. Diabetes, 2002, 9(1), 87-98.
[3] Webb, A.R.; DeCosta, B.R.; Holick, M.F. Sunlight regulates the cutaneous production of vitamin D3 by causing its photodegradation. J. Clin. Endocrinol. Metab, 1989, 68(5), 882-887.
[4] Holick, M.F. McCollum Award Lecture, 1994: vitamin D--new horizons for the 21st century. Am. J. Clin. Nutr1994, 60(4), 619630.
[5] Zittermann, A. The estimated benefits of vitamin D for Germany. Mol. Nutr. Food. Res, 2010, 54(8), 1164-1171.
[6] Deutch, B.; Dyerberg, J.; Pedersen, H.S.; Aschlund, E.; Hansen, J.C. Traditional and modern Greenlandic food - dietary composition, nutrients and contaminants. Sci. Total. Environ., 2007, 384(1-3), 106-119.
[7] Holick, M.F. Vitamin D deficiency. New. Engl. J. Med., 2007, 557(3), 266-281.
[8] Vieth, R. Critique of the considerations for establishing the upper tolerable intake level for vitamin D: Critical need for revisionupwards. J. Nutr., 2006, 136(4), 1117-1122.
[9] Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J.; IOF Committee of Scientific Advisors (CSA) Nutrition Working Group. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int., 2009, 20(11), 1807-1820.
[10] Ziegler, R.; Minne, H.; Raue, F.; Paar, G.; Delling, G. Observations in vitamin D and dihydrotachysterol poisoning. Dtsch. Med. Wochenschr., 1975, 100(9), 415-423. *[Article in German]
[II] Lilienfeld-Toal, H.V.; Messerschmidt, W.; Sturm, B.; Ochs, H. 25-hydroxy-vitamin D levels in a patient with hypervitaminosis D. Klin. Wochenschr., 1978, 56(14), 715-717. *[Article in German]
[12] Koutka, P.; Chen, T.C.; Holick, M.F. Vitamin D intoxication associated with an over-the-counter supplement. New. Engl. J. Med., 2001, 345(1), 66-67.
[13] Araki, T.; Holick, M.F.; Alfonso, B.D.; Charlap, E.; Romero, C.M.; Rizk, D.; Newman, L.G. Vitamin D intoxication with severe hypercalcemia due to manufacturing and labeling errors of two dietary supplements made in the United States. J. Clin. Endocrinol. Metab., 2011, 96(12), 3603-3608.
[14] Jacobus, C.H.; Holick, M.F.; Shao, Q.; Chen, T.C.; Holm, I.A.; Kolodny, J.M.; Fuleihan, G.E.; Seely, E.W. Hypervitaminosis D associated with drinking milk. New. Engl. J. Med., 1992, 30(18), 1173-1177.
[15] Blank, S.; Scanlon, K.S.; Sinks, T.H.; Lett, S.; Falk, H. An outbreak of hypervitaminosis D associated with the overfortification of milk from a home-delivery dairy. Am. J. Public Health, 1995, 85(5),656-659.
[16] Chesney, R.W. Vitamin D: Can an upper limit be defined? J. Nutr., 1989, 119(12 Suppl), 1825-8.
[17] Markestad, T.; Hesse, V.; Siebenhuner, M.; Jahreis, G.; Aksnes, L.; Plenert, W.; Aarskog, D. Intermittent high-dose vitamin D prophylaxis during infancy: effect on vitamin D metabolites, calcium, and phosphorus. Am. J. Clin. Nutr., 1987, 46(4), 652-658.
[18] Kobylinski, S.; Hafer, B.; Kohde, G. *[Correlative pathologic studies on the role of vitamin D in vascular calcinosis in childhood]. Zentralbl. Allg. Pathol., 1984, 129(2), 137-147. Article in German
[19] Deluca, H.F.; Prahl, J.M.; Plum, L.A. 1,25-Dihydroxyvitamin D is not responsible for toxicity caused by vitamin D or 25-hydroxyvitamin D. Arch. Biochem. Biophys., 2011, 505(2), 226230.
[20] IOM (Institute of Medicine). Dietary Reference Intakes for Calcium and Vitamin D. The National Academies Press: Washington, DC, 2011
[21] Price, P.A.; Buckley, J.R.; Williamson, M.K. The amino bisphosphonate ibandronate prevents vitamin D toxicity and inhibits vitamin D-induced calcification of arteries, cartilage, lungs and kidneys in rats. J. Nutr., 2001, 131(11), 2910-2915.
[22] Jones, G. Pharmacokinetics of vitamin D toxicity. Am. J. Clin. Nutr., 2008, 88(2), 582S-586S.
[23] Tuohimaa, P. Vitamin D and aging. J. Steroid. Biochem. Mol. Biol., 2009, 114(1-2), 78-84. *[24] Sharma, O.P. Vitamin D, calcium, and sarcoidosis. Chest., 1996, 109(2), 535-539.
[25] Plum, L.A.; DeLuca, H.F. Vitamin D, disease and therapeutic opportunities. Nature Rev. Drug. Discov., 2010, 9(12), 941-955.
[26] Hathcock, J.N.; Shao, A.; Vieth, R.; Heaney, R. Risk assessment for vitamin D. Am. J. Clin. Nutr., 2007, 85(1), 6-18.
[27] Heaney, R.P.; Davies, K.M.; Chen, T.C.; Holick, M.F.; Barger-Lux, M.J. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr., 2003, 77(1), 204-210.
[28] Barger-Lux, M.J.; Heaney, R.P. Effects of above average summer sun exposure on serum 25-hydroxyvitamin D and calcium absorption. J. Clin. Endocrinol. Metab., 2002, 87(11), 4952-4956.
[29] Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; Mayne, S.T.; Rosen, C.J.; Shapses, S.A. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J. Clin. Endocrinol. Metab, 2011, 96(1), 53-58.
[30] Hypponen, E.; Berry, D.J.; Wjst, M.; Power, C. Serum 25-hydroxyvitamin D and IgE - a significant but nonlinear relationship. Allergy, 2009, 64(4), 613-620.
[31] Zittermann, A.; Borgermann, J.; Gummert, J.F.; Pilz, S. Future directions in cardiovascular research. Nutr. Metab. Cardiovasc. Dis., 2012, 22(7), 541-546.
[32] Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial. JAMA, 2010, 303(18), 1815-1822.
[33] Rossini, M.; Gatti, D.; Viapiana, O.; Fracassi, E.; Idolazzi, L.; Zanoni, S.; Adami, S. Short-Term Effects on Bone Turnover Markers of a Single High Dose of Oral Vitamin D3. J. Clin. Endocrinol. Metab., 2012, 97(4), E622-E626.
[34] Trivedi, D.P.; Doll, R.; Khaw, K.T. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ, 2003, 326(7387), 469.
[35] Vieth, R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am. J. Clin. Nutr., 1999, 69(5), 842-856.
[36] Maalouf, J.; Nabulsi, M.; Vieth, R.; Kimball, S.; El-Rassi, R.; Mahfoud, Z.; El-Hajj Fuleihan, G. Short- and long-term safety of weekly high-dose vitamin D3 supplementation in school children. J. Clin. Endocrinol. Metab., 2008, 93(7), 2693-2701.
[37] Sneve, M.; Figenschau, Y.; Jorde, R. Supplementation with cholecalciferol does not result in weight reduction in overweight and obese subjects. Eur. J. Endocrinol., 2008, 159(6), 675-684. *[38] Zittermann, A.; Frisch, S.; Berthold, H.K.; Gotting, C.; Kuhn, J.; Kleesiek, K.; Stehle, P.; Koertke, H.; Koerfer, R. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am. J. Clin. Nutr., 2009, 89(5), 1321-1327.
[39] Mocanu, V.; Stitt, P.A.; Costan, A.R.; Voroniuc, O.; Zbranca, E.; Luca, V.; Vieth, R. Long-term effects of giving nursing home residents bread fortified with 125 microg (5000 IU) vitamin D(3) per daily serving. Am. J. Clin. Nutr, 2009, 89(4), 1132-1137.
[40] von Hurst, P.R.; Stonehouse, W.; Coad, J. Vitamin D supplementation reduces insulin resistance in South Asian women living in New Zealand who are insulin resistant and vitamin D deficient - a randomised, placebo-controlled trial. Br. J. Nutr., 2010, 103(4), 549-555.
[41] Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr., 2006, 84(1), 18-28.
[42] Bischoff-Ferrari, H.A.; Shao, A.; Dawson-Hughes, B.; Hathcock, J.; Giovannucci, E.; Willett, W.C. Benefit-risk assessment of vitamin D supplementation. Osteoporos. Int., 2010, 21(7), 11211132.
[43] Zittermann, A.; Iodice, S.; Pilz, S.; Grant, W.B.; Bagnardi, V.; Gandini, S. Vitamin D deficiency and mortality risk in the general population: a meta-analysis of prospective cohort studies. Am. J. Clin. Nutr, 2012, 95(1), 91-100.
[44] Zittermann, A. Serum 25-hydroxyvitamin D response to oral vitamin D intake in children. Am. J. Clin. Nutr., 2003, 78(3), 496-497.
[45] Schleithoff, S.S.; Zittermann, A.; Tenderich, G.; Berthold, H.K.; Stehle, P.; Koerfer, R. Vitamin D supplementation improves cytokine profiles in patients with congestive heart failure: a double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr., 2006, 83(4), 754-759.
[46] Wagner, C.L.; Howard, C.; Hulsey, T.C.; Lawrence, R.A.; Taylor, S.N.; Will, H.; Ebeling, M.; Hutson, J.; Hollis, B.W. Circulating 25-hydroxyvitamin d levels in fully breastfed infants on oral vitamin d supplementation. Int. J. Endocrinol., 2010, 2010, 235035.
[47] Aloia, J.F.; Patel, M.; Dimaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr., 2008, 87(6), 1952-1958.
[48] Lips, P.; Duong, T.; Oleksik, A.; Black, D.; Cummings, S.; Cox, D.; Nickelsen, T. A global study of vitamin D status and parathyroid function in postmenopausal women with osteoporosis: baseline data from the multiple outcomes of raloxifene evaluation clinical trial. J. Clin. Endocrinol. Metab., 2001, 86(3), 1212-1221.
[49] Houghton, L.A.; Vieth, R. The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am. J. Clin. Nutr., 2006, 84(4), 694-697.
[50] Vieth, R. The pharmamincology of vitamin D, including fortification strategies. In: Vitamin D. Second edition. Feldman D, Pike JW, Glorieux FH (Eds). Elsevier Academic Press, Amsterdam, 2005, pp. 995-1015.
[51] Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stocklin, E.; Sidelnikov, E.; Willett, W.C.; Orav, E.J.; Stahelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; Henschkowski, J.; von Eckardstein, A.; Egli, A. Oral supplementation with 25(OH)D(3) versus vitamin D(3) : effects on 25(OH)D levels, lower extremity function, blood pressure and markers of innate immunity. J. Bone. Miner. Res., 2011, doi: 10.1002/jbmr.551. [Epub ahead of print]
[52] Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of daily, weekly, and monthly vitamin D3 in ethanol dosing protocols for two months in elderly hip fracture patients. J. Clin Endocrinol. Metab., 2008, 93(9), 3430-3405.
[53] van Groningen, L.; Opdenoordt, S.; van Sorge, A.; Telting, D.; Giesen, A.; de Boer, H. Cholecalciferol loading dose guideline for vitamin D-deficient adults. Eur. J. Endocrinol. 2010, 162(4), 805-811.
Short URL = http://is.gd/safety_VitD