Vitamin D Resistance: video Dr. Cheng
73 minute YouTube interview
Sample of charts
Summary by Google AI Dec 2025
Vitamin D as a Master Regulator (05:51): Dr. Cheng emphasizes that Vitamin D is actually a hormone and systems regulator, not just a nutrient for bones. It influences thousands of genes across various physiological functions, including immune competence, insulin signaling, and metabolic flexibility.
Optimal Blood Levels vs. "Passing Grades" (09:20): While conventional medicine often aims for 30 ng/mL, Dr. Cheng views this as merely a "passing grade." He recommends an optimal range of 50–100 ng/mL for most adults, noting that effectiveness rises sharply in this window with a high safety profile.
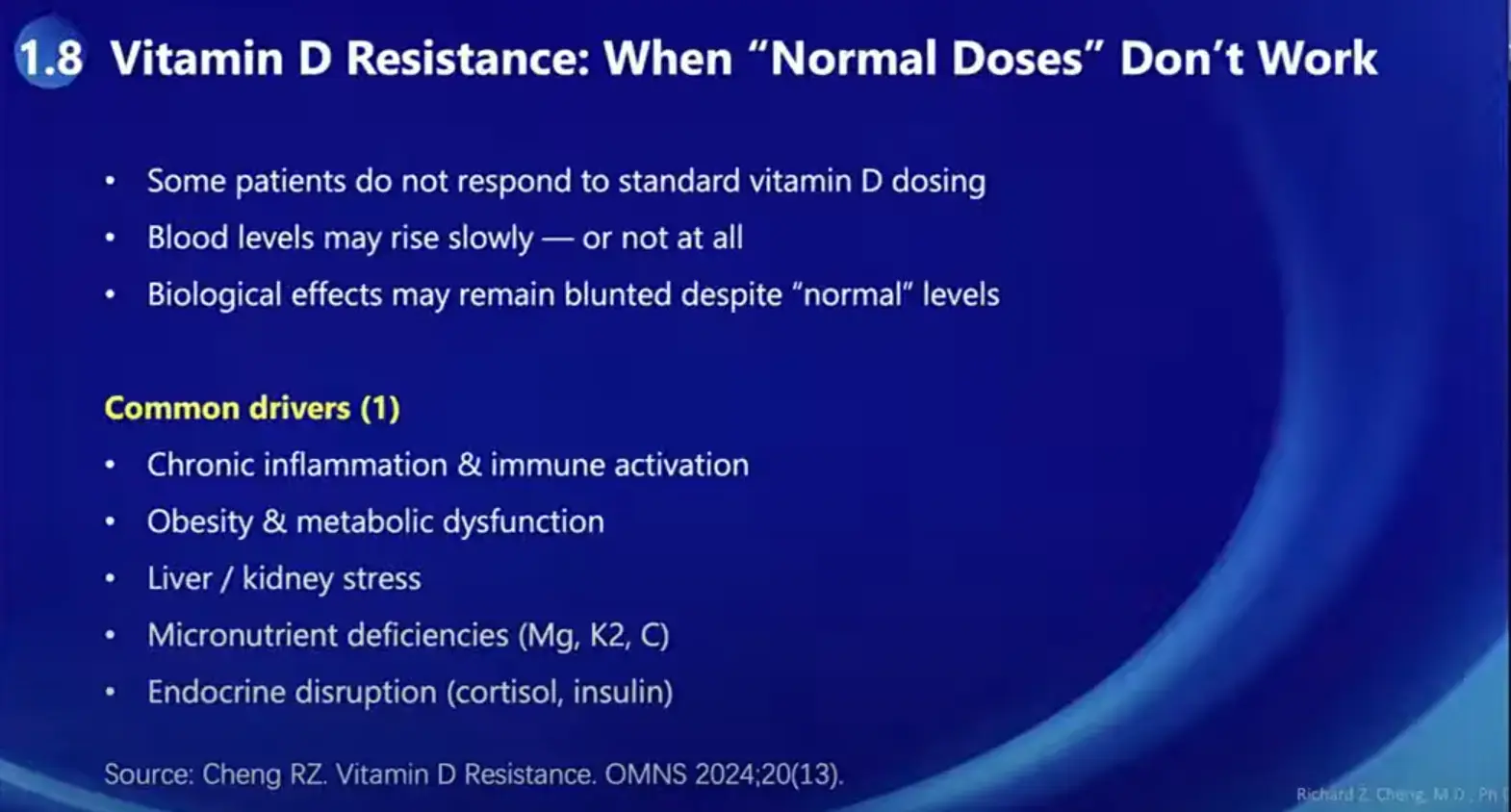
Understanding Vitamin D Resistance (18:05): Resistance occurs when typical doses fail to produce the expected biological effect. This can be caused by genetic variants (162 identified variants), chronic inflammation, obesity, and gut issues like leaky gut or dysbiosis, which block the Vitamin D Receptor (VDR).
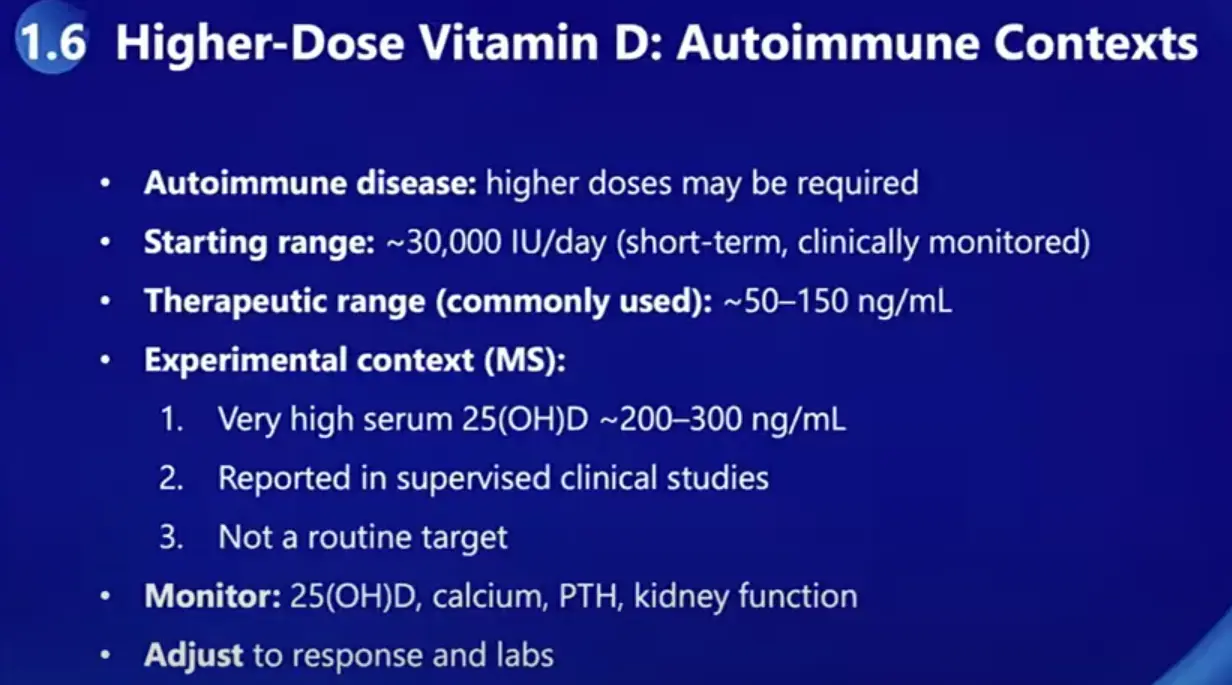
High-Dose Protocols for Autoimmunity (16:00): For autoimmune conditions like Multiple Sclerosis or Lupus, Dr. Cheng utilizes high-dose protocols (starting at 30,000 IU/day), often referred to as the Coimbra Protocol. He notes that these patients require significantly higher levels (sometimes up to 250 ng/mL) to overcome resistance, provided they are supervised to monitor calcium and kidney function.
Synergy with Magnesium and Vitamin K2 (53:53): Vitamin D should never be taken in isolation. Magnesium is essential as it relaxes cells and acts as a natural antagonist to calcium, while Vitamin K2 is critical for preventing calcium from depositing in soft tissues like arteries. Dr. Cheng personally takes 45mg of K2 daily for its bone and cardiovascular benefits.
The "ICV Axis" and Hormonal Balance (24:39): Dr. Cheng introduces the Insulin-Cortisol-Vitamin C/D (ICV) axis as a foundational regulatory system. He argues that functional resistance to Vitamin D is often tied to dysfunctions in insulin and cortisol, making it impossible to balance hormones without addressing these root drivers first.
Root Cause Medicine over Symptom Management (32:58): He critiques modern medicine for focusing on "hallmarks" (mechanisms) rather than "root drivers." His protocol follows an "OM Blueprint": lifestyle first (low-carb diet, exercise), followed by correcting nutritional deficiencies, then detoxification, and finally advanced regenerative therapies.
The 10 Root Drivers of Disease: Relevant Glasp insights clarify Dr. Cheng's framework for health, which identifies 10 primary drivers of chronic illness: 1) Genetic/Epigenetic, 2) Micronutrient Deficiency,[1] 3) Toxin Overload, 4) Hormonal Imbalance,[1] 5) Chronic Infection,[2] 6) Gut Health, 7) Mitochondrial Dysfunction, 8) Chronic Inflammation, 9) Oxidative Stress, and 10) Mind-Body-Spirit (Source).
Timestanps (not hyperlinked)
00:00 – 00:25 | Welcome & Introduction to Vitamin D Study Hour
00:25 – 00:04:13 | Dr. Richard Cheng Introduction & Background
00:04:13 – 00:05:10 | Opening Remarks & Slide Setup
00:05:10 – 00:07:30 | Vitamin D as a Hormone & Systems Regulator 00:07:30 – 00:10:15 | Vitamin D Deficiency & Disease Risk
00:10:15 – 00:16:00 | Optimal Vitamin D Levels, Effectiveness & Safety
00:16:00 – 00:19:30 | Dosing Strategies & Individual Variability
00:19:30 – 00:23:20 | High-Dose Vitamin D & Autoimmune Disease (Coimbra Protocol)
00:23:20 – 00:27:30 | What Is Vitamin D Resistance?
00:27:30 – 00:30:20 | Genetic Variants Affecting Vitamin D Status
00:30:20 – 00:34:20 | Hormones, ICV Axis & Nutrient Interactions
00:34:20 – 00:38:30 | Clinical Case Examples & Blood Level Differences
00:38:30 – 00:43:00 | Conventional Medicine vs Root-Cause Medicine
00:43:00 – 00:47:00 | Cancer, Aging & Hallmarks vs Root Drivers
00:47:00 – 00:51:55 | Integrative Orthomolecular Medicine (IOM) Blueprint
00:51:55 – 00:53:05 | Transition to Live Q&A
00:53:05 – 00:56:15 | Vitamin D Resistance, Magnesium & Inflammation
00:56:15 – 00:59:55 | Vitamin A, RXR Competition & Vitamin D Function
00:59:55 – 01:02:55 | Vitamin D, Melatonin & Sleep
01:02:55 – 01:06:35 | Magnesium, Vitamin K2 & Calcium Balance
01:06:35 – 01:09:20 | Practitioner Guidance & Clinical Training
01:09:20 – 01:11:20 | Optimal Vitamin D for Chronic Disease & Aging
01:11:20 – 01:12:41 | Final Thoughts & Closing Remarks
Related in VitaminDWiki
- Orthomolecular Vitamin D Resistance same author
- Vitamin D: 40-70 ng is optimal, sometimes more is needed - Grant, Sunil, Pawel, Cheng
Full transcipt
(00:08) Hello everyone and welcome to another vitamin D study hour and today I am excited to have Dr. Richard Chang here with us and um he's going to be discussing the topic of understanding and addressing vitamin D resistance. Um hopefully you can see my screen. Does that look good to you, Dr. Chang? >> Yeah, I can see that. Hi, everybody.
(00:34) >> Okay. All right. So, uh, just a quick introduction to Dr. Chang. Um, first off, thank you so much for being here today. I'm really excited to cover this topic. Uh, so Dr. Chang is a medical doctor and has a PhD. He is a practicing physician in both the United States as well as China.
(00:56) Um he has his PhD in biochemistry and molecular bi biology. Um he is a hall of fame inductee of the international society for orthomolecular medicine and a fellow of the American Academy of anti-aging and regenerative medicine. He is also the founder and director of Chang Integrative Health Center in Shanghai and co-founder of the China Low Carb Medicine Alliance.
(01:21) Um he is a recognized um he's recognized internationally for his work in integrative medicine and ortho orthomolecular therapy and he is the editor and chief of the orthomolecular medicine news service. Um so today uh we are going to be covering um the topic like I said of vitamin D resistance and we're going to be focusing on a paper that Dr. Chang recently wrote, "Underst understanding and addressing vitamin D resistance, a comprehensive approach integrating genetic, environmental, and nutritional factors." And we're also going to be referring to a recently published paper uh genomewide uh gene environment interaction study uncovers 162 vitamin D status variants. So uh that's uh posted to our website grassrootsalth.net.
(02:11) And I do want to mention real quick, you know, we we put these papers out ahead of time as optional homework. And I got to say I thank you to those who sent questions and comments in uh who actually did read the papers and had questions specifically about the papers. So I really appreciate that you guys have been putting your attention on uh this uh this homework beforehand.
(02:37) So before I hand the uh presentation over to Dr. Chang, just a couple reminders. Um, please submit your questions to the Q&A box and all questions will be answered after the study review. Um, those that were submitted prior to the webinar will be uh addressed first and yes, this will be recorded and posted to our website and to YouTube at a later date.
(03:05) So, as most of you know, Grassroots Health has been running an online study on vitamin D for um since 2008, and you can get a vitamin D test kit, so you can measure your vitamin D levels from home. Um it is a self-sponsored study, and that is how Grassroots Health can fund its operations, and we appreciate those of you who participate.
(03:29) And then uh finally our next uh vitamin D study hours will be uh on the 7th of January is our next one with Dr. Hollik addressing the confusing guidelines that we have to deal with these days on vitamin D and that is followed by Dr. Barbara Buché who will be presenting on the 21st on metabolic syndrome, insulin resistance and type 2 diabetes.
(03:56) So, please email me, jengrasshealth.org if you have questions, if you have testimonials and thank you to those uh organizations that support us. And with that, I am going to hand this over to Dr. Chang while I get his slides set up. >> Welcome Dr. Chang. >> Hi, thank you. Thank you Jane again for the invitation and also appreciate the work the grassroots and you under your leadership has been doing.
(04:28) It's uh really helpful for promoting true health. >> Well, we're uh doing this with the help of you and many other other of our uh vitamin D scientists. So, I certainly certainly appreciate you joining us and I appreciate all the work that you're doing. Um, all right. So, let me just get Can you see your slides? Okay.
(04:50) >> Yes, I can see it. I can see it. >> Great. >> All right. Just tell me when to move on. >> All right. Go on. Let's start. Uh, well, this is my uh bio, but uh we can skip this one. Um well one thing I want to mention about uh recently I'm also invited to join the board of directors of uh the realen clinic and that's quite an honor which uh many of you probably know which is the world's pioneer with over 40 years of experiencing highdose vitamin C another critical nutrient to our health uh and also another thing interesting thing is I was invited to join the South Carolina State Medical Board of Reviewers and Board of Examiners as a expert reviewer. And I told them when they did it, I said, "I'm not one of your regular guys." I said, you know, because I didn't want to get into arguments or try. They said, "Yes, exactly. You're the type of experts we need.
(05:51) " So that shows the direction or at least part of the direction that uh American healthcare is going towards hopefully. Yeah. Go on. Yeah. Oh, okay. So uh is that first one or the second one? Uh I think there there should be another one. The go back go back one. Yeah. Okay. Yeah. Well, first of all, vitamin D and as many of you know about vitamin D and uh you know we used to think vitamin D is about the bone and as I mean bone, but it's a lot more than a uh just a bone nutrient.
(06:29) So basically this vitamin D is not actually it's not really a vitamin it is a hormone as we know and it is a systems regulator. It affects every organ every cell in our body literally everyone. Okay. So uh as uh pointed out Jang just mentioned in a recent paper again is that you know vitamin D regulates thousands of genes across every spectrum of physiological functions.
(07:00) So uh and also important for not only for the bone but also physiological network immune competence insulin signaling and metabolic flexibility information redux you name it you you name it you got it you know. It's widespread. Okay, next one. So we know vitamin D deficiency as you know as vitamin D is a critical part of our normal physiology the its deficiency is a major root driver of all diseases not just chronic but also acute as we have seen we witnessed during covid-19 you know where part of my cocktail integrative also medicine cocktail is high vitamin D I often times give 50,000 units every day for like seven days to 10 days and then and then went off uh to regular dose and it as part of the cocktail it saved many patients from severe symptoms and even rescued people from ICU. Okay, next one. Well, like I mentioned the vitamin D is a systems signal.
(08:11) Okay, we should consider it as ma one of the master regulators of our physiology. It's involved including in ASCVD basically the astroscerotic cardiovascular diseases like coronary heart disease which is the top killer worldwide at least in the developed nations and which is also one of the most interested areas for myself because simply I don't want to die of ASVD and also in cancer and in autoimmune diseases.
(08:43) Next. Well, this is a summary. Okay, we have so many studies on vitamin D and I I reviewed I thank you for your uh questions you sent in advance about vitamin D dozing, side effects, optimal range and these are common questions that we all do particularly clinicians including myself. So this is a summary of these studies and also my view personal perspective in in my uh you know in M framework.
(09:20) Basically vitamin D seems to have a you know the blue curve here shows the effectiveness. Okay, clearly we know under 20 nanogram per meal as the regular guideline says is deficient of vitamin D and the vitamin D effects rise very sharply between you know the low level to maybe ac close to 50 60 70 80 range gradually it slows down.
(09:50) So and this is the effectiveness up to now the literature seems to suggest that once you approach probably 70 80 nanog per meal level your uh you that's where probably you get most of your benefits and after that you still have gain but a little bit less of the results I mean uh maximum effects and the side effects don't really show up until above 150 for sure and uh probably after 200 more significantly.
(10:27) So my interpretation of the data and summarized on this graph is that uh seems to be that vitamin D doses between 50 and 150 is the is the wide windows of effectiveness and the safety. Okay, within this range it's I feel quite comfortable. Normally we of of course we say we keep it anywhere between 40 and 50 nanogram and 100 nanog per meal.
(10:57) Okay, no side effects as far as I know uh has been reported uh in the literature with a vitamin D you know within this range. Yeah, if uh anything okay I'd like to know and u here I I want to raise one important question interesting question it's a philosophical common sense issue okay we know the endocrine society's guideline and that's a lot of conventional doctors mentioning is that they want to keep vitamin D at 30 nanog and above right that's the guideline the issue here is that we do know that above 30 nanog appears to be sort of the bottom line of the normal range you begin to see effects okay however that's not the maximum uh benefits of vitamin D is okay so lot of doctors in practice today particularly conventional medicine doctors they sort of aim vitamin D many of them don't even do that but they aim to keep vitamin D up at the 30 nanog here is a question 30 n is like a passing line.
(12:10) Okay, most of us, you know, we all have gone through schools and let's say in the school system, I mean, when I was growing up, we had a grading system of 60 points out of 100. 60 is passing 100 is is the maximum. Nobody, it's common sense. Nobody is satisfied with 60 because everybody is aiming for 100. Okay? So why in the world here in medicine we would aim for passing grade which is 30 nanog which is like 60 equivalent in a scale of 0 to 100 and that's shouldn't we think about it so I'm not looking for only the passing grade of vitamin D 30 nanogram
(12:49) I'm looking for what's the maximum that I personally can do for myself and for my patients okay so my answer here is that appears to Now here's another question is that I'm going to I have one slide showing that is that now we do know with the existing data vitamin D is quite safe at least up to 100 nanog okay even above 100 basically 100 to 150 it's still quite safe of course you know a lot of people are very uh concerned about going into that range and of course I would say I would add what I've been recommending Meaning is that keep it between 50 and 100 nanog no question don't ask I'm I'm willing to debate against anybody in any court of law okay on this going above 100 yeah sure I would always add a caution I said use it under the supervision of a qualified and experienced healthcare provider okay so that's my view keep it between 50 and 100 for between 100 and 150 that's a little bit of wing window of like a supervision is required.
(14:03) That's where I would put the certain disease condition patients particularly autoimmune diseases. We don't know about cancer, heart disease, disease, whether higher doses are more effective. We don't know the answer yet. And particularly aging and of course obviously I'm getting hold of interest in anti-aging. Do higher levels of vitamin D, for example, between 100 and 150 uh have more effects in anti-aging than between 50 and 100? I don't know the answer.
(14:33) I don't know the answer to that. Okay. But uh that's an interesting area to search. But I right now I don't you know we don't really recommend going above 150. And I have one slide showing in autoimmune diseases for example multiple scerosis. There are some small I mean there are some clinical trials uh shooting for higher like 200 even 300 u nanogram but uh that's with extra caution.
(14:59) Okay let's move on next. Okay so basically it's already summarized here. So uh uh between 50 and 100 nanog no questions asked and to achieve this level that's the question and everybody is a little bit different in my view and my clinical experience and some of the literature reported in papers between 5,000 to 10,000 IU a day of vitamin D3 is I feel very comfortable.
(15:30) I don't I don't even worry about I tell everybody go home do it any problem I'm willing to go to court with you don't worry about it and so uh of course special conditions like obesity inflammation you know uh the other conditions may need may need more and we will talk a little bit more later. So the key here is that uh the doses and the blood levels do not have a linear uh they don't always correlate uh different people different conditions different season like winter in northern hemisphere right now we may need a little bit more vitamin D I go a little bit higher for myself and uh of course we need to measure we need to adjust we need to check periodically next okay we just mentioned about autoimmune disease And as we all know about more than 10 maybe 13 12 years ago Dr. Coinbar from I think what Brazil South America man proposed a coinbar protocol basically highdose vitamin D appears to be uh helpful effective in autoimmune diseases and so this is what I do uh we usually I usually start with 30,000 IU a day and uh I measure their vitamin D level in two to three months because it takes a little bit time for vitamin D to saturate our uh fat tissue or Vitamin D is a fat soluble uh agent. It takes some time to saturate all the fat cells in our body and to reach a steady state level. It we may vary between like two three months. Okay. So we usually measure at the same time uh I mention here we also measure particularly for highdose range we measure vitamin D level of course calcium parasy hormone kidney functions and I may even you know creatinine b and sometimes I even add ultrasound making sure there's no calcium crystalline formation in the kidney and of course we advise people to stay away from calcium high calcium foods or calcium supplements and uh drink a lot of And so that's uh that is uh the autoimmune approach as as I mentioned here in some cases reporting uh supervised clinical studies 200 300 nanogram per meal has been used for short term. Okay. All right.
(18:05) Next slide. Uh is is this next? Yeah. Okay. Well, so one question is why autoimmunity requires high vitamin D doses? That's an interesting question. As uh Jane put out up front and also in advance of of those papers. One of the papers about vitamin D resistance and we know autoimmune diseases. Uh let me briefly uh explain a little bit autoimmunity in my uh my understanding of it.
(18:36) Autoimmunity is a typical multi-organ disease. It's probably one of the best reflections of our poor lifestyle. Okay. My interpretation as many of you are probably well aware of is that usually these diseases starts these this disease start from the gut. Okay, we know about leaky gut. We know about this biosis. I'm not going to go into detail.
(18:59) Basically all these unhealthy diets, the dietary toxins, offending agents, you know, imbal unbalanced bacterium, they create a leaky gut, a basically our weakened uh gut uh protective layer. So this allows the leaky gut and this biosis actually this biosis is part of the leaky gut we can call it syndrome. Okay.
(19:28) So basically that condition allows undigested or partially digested food food stuff as well as of toxins microorganism bacteria virus these things to enter through our gut barrier into our body that's the bottom line for a healthy person these things normally are not permitted inside I mean in in through our gut into system. Okay, that's what our gut is like our skin.
(19:58) Our skin protects our inside body from the outside you know invaders. So because of that the leaky gut undigested or these virus all the other toxin can enter our system and these are highly antigen antigenic. they can cause immune reactions and that causes the uh you know complicated very convoluted immune reactions we classify into so many different types okay the mechanisms but bottom line is it starts from poor health and this actually interestingly reminds me one of the after I actually accidentally helped quite a few skin rash patients I should have put some uh cases here today I didn't But u in my career I have cured uh several skin rash diseases notably uh anyway psoriasis. The my first case was psoriasis and then that reminded me of a medical school professor who taught us over 40 years ago. I I I entered medicine 50 years ago.
(21:06) He was saying a good dermatologist needs to be a good internist first. I remember that clearly. I never understood it not until recently the last within the last 10 15 years then I realized yes actually a lot of the skin diseases actually are a reflection of our internal medical problems particularly gut so coming back to autoimmune disease so basically in my view the root cause lies in the gut okay what does that mean what I said is that autoimmunity itself is a inflammatory disease no question there And it's a gut dispiosis, leaky gut issue. It's a uh poor vitamin, you know, nutrition issue. It's a toxic, you know, highly uh, you know, toxin overload issue. So those are all the conditions that will increase your, you know, vitamin D resistance as I described in that in that article. Okay, that's probably probably why autoimmunity uh patients require higher vitamin D doses because there are so many other factors that are affecting the vitamin D uh receptors, vitamin D absorption and vitamin D physiological functions in addition to the genetics.
(22:25) Okay. And next one. So the message here is that the vitamin D resistance the normal doses don't always work. So that's another question and how do we you know make a judgment? How do we judge in clinical medicine whether a patient is uh has sufficient level of vitamin D? Blood level obviously is the main is still the main stay.
(22:54) we measure the blood level but also I would recommend combined the clinical uh uh scenario. Okay. If the patient shows you know very safe profile on vitamin D, no issues I as I mentioned no issue of high calcium uh problems and for example certain special diseases you may gradually increase vitamin D doses until basically try to adjust for the physiological response to see where is the sweet spot or the better you know dose responsive range for that particular patient. Okay.
(23:30) So normal dose doesn't always mean good personal uh level for that particular person. Next. Well, this is a summary of uh what the recent uh uh the genetic uh study Jang mentioned up front is they studied I mean they found about more than about 160 was 162 genetic variants that regulated vitamin D across the entire pathway.
(24:02) Basically it affect these variants affect the various levels of skin synthesis liver can activation of vitamin D and transport a bioavailability bio availability you know the basically whether our body can use and every individual cell can use the vitamin D or not and also the vitamin D receptor signaling. So, so this is explains again from the genetic level why everybody responds a little bit differently and every person at different age different state probably even different season may respond differently next and also here I want to show one of our recent papers which I uh we don't have time to go into detail but I just want to mention here uh the ICV axis the I stands for insulin C for cortisol and vitamin C for V for vitamin C. Basically, this idea originally came from Dr. Levy, Tom Levy, and he published one article on our awesome molecular.net.
(25:03) Basically, our awesome molecular medicine news service. If you have not subscribed, subscribe to that. It's free. I advise everybody should because uh we publish really interesting uh articles there. And so, he published one article about cortisol and vitamin C. And during a recent conference in cancer care reimagining in in real clinic we uh Tom Levy and I and Dr. Ron Honeyhacki the CMO of the real clinic we went into further discussion and I felt uh I propose actually this is probably more important basically the ICV access also ties into our PHR. Many of you probably uh are familiar with the bio identical hormone replacement basically hormone balance. We know in BHR the hormone balance thyroid is the starting point that's very critical and now we believe that actually thyroid probably is not really the first we should start from ICV.
(26:03) The insulin ties into today's widespread obesity overweight insulin resistance issue. That's a bottom path pathology practically for a lot of people America in particular I think uh probably 80 about 80% of people here in this country we have this issue maybe more than that actually anyway so here I show you I'm not going to quot the article we publish here as you in reference number one published in the preprints uh I'm trying to have it published in the academic journal now because I believe this IV CV access would have a huge impact in functional medicine because you can't balance hormones without a balanced thyroid without a balanced ICV axis. Okay, that's that's quite critical here. But here I want to show you is that actually ICV dysfunction affects functional dresistance as we're discussing these two papers. Okay, that's interesting that ties neatly into this uh hormone uh balance uh system again. Okay, next please.
(27:11) Okay, so this is a summary and with some cases showing you how different different dose having different blood levels. The first two are from James, you know, uh the grassroots uh uh study. Basically, she she they reported the couple husband, I'm sure you are all familiar with this is the husband and wife both take 2,000 IU a day.
(27:38) The wife was within like a 40 to 60 nanog and but the husband was only less than 20 with the same 2,000. And so the husband needed to take 10 times more doses to reach 30 to 40 level. Basically the husband takes more 10 times more than the wife. That's a very good example actually and that shows you many other conditions affect the blood level of vitamin D.
(28:07) And the second the last two are my personal case. I just highlighted two of them here. One is one of them is my recent case is a 60 some year man basically like like you know one regular Jew on the street 60 some year old was early level of astroscerosis and he wants a better care so came to my condition healthcare basically primarily for ASVD prevention he has some coroted you know artery issues so I gave him my integrative also malle medicine uh I call it the protocol which I will talk a little bit later and uh but he inadvertently took 30,000 IU vitamin D a day for a month and I didn't know that I asked him to take a 10,000 well I said don't worry I said let's go check uh he he he asked whether he should be I said don't I said check the check blood level and do the clinical work which we did well sure enough his vitamin D was 118 nanogram a little bit above 00. Okay.
(29:10) But not not too bad. And also he didn't have any hypocalcemia, no renal function issues, no piatry issues. Everything was fine. Okay. That's 30,000 units a day for for 30 days, for a month. Uh he says, "Now we have another patient and this patient that's not my patient until later.
(29:31) Basically, the mother was concerned about the son. The son was I think 20ome years old and and she was giving him 50,000 units every day for I think like two three months and then uh they did some blood work found that the blood vitamin D was more than 200 nanogram per meal also he showed the hypocalcemia and the acute phase renal function basic acute kidney injury okay so everybody is a little bit different of course you know so that shows you uh the doses you know here but in general for uh I recommend 5,000 to 10,000 units to practically every adult and no no questions asked you know I don't worry about any overdose there okay next okay so uh up till now I sort of that's my summary of my take uh in vitamin D in a common sense style and let me just summarize there is yes the vitamin D a lot of mechanisms a lot of other issues involved as I summarized you know basically regardless of the health conditions disease whatever I put I mean to 50 200 nanogram per meal that's my target and as a clinician I care more about clinical you know outcome rather than you know the mechanisms the why the reasoning is all helping us to form the conclusion and to safely manage patient. So uh 50 to 100 nanogram for autoimmune disease patients I would push 400 to 250 of course monitor okay for individual patients I may even push higher and so that's the bottom line of my take on vitamin D okay now uh should I take a break or should I go on for the second part okay I will go on so now I will talk a little bit let's go back to the uh go to the two one uh the first the other slide. Yeah.
(31:35) Basically in my 50 years clinical history and I mean clinical medical career. So my again is you know I uh you know I'm a clinician. I want to you know myself to be healthy and anti-aging and I want patients better. Okay. So here first few slides I want to summarize my view on conventional medicine. This is a good it's a we know blind people feeling the elephant right everybody feels part of it okay next but we're not seeing the whole patient you know this is another view you know uh basically here today's medicine as you we all know is that actually they directly there's something called translational medicine trans translational medicine today I think it's m misinterpreted is that they directly translate the lab research into clinic uh clinical medicine basically one drug. Okay, you know we do need a basic research as shown here represented by this uh pretty lady here looking through a microscope.
(32:36) For basic scientists, we need that. I did that too for my PhD. We need to break down the complex systems into parts and study mechanisms. We need to know why. But important as a clinician, we need a holistic view. We are not treating mechanisms. We are treating the patient. That's the problem. That's the her point here.
(32:58) Okay? Because conventional medicine today they confuse the two I whether intentionally or unintentionally okay a lot of it I believe is intentional okay so today's problem is that if we through you know but anyway summarize here if we treat a patient through a micros microscopic view we mess up okay next so this is summary I'm not going to go over the detail but it's a summary between the conventional medicine and what I call integrated also molecular medicine or actually the true medicine should be okay so roughly is that here is summarity is that we need to treat
(33:39) root causes what is the ultimate root let me tell you this even among the functional medicine alternative care medicine scientists and doctors I feel a lot of them missing this point we are so used to dive deep into the mechanisms. Okay, I used to do the same when I was a younger doctor.
(34:07) I had my hands behind my back, the nose, you know, eye to the ceiling, you know, very arrogant, very proud. I'm a proud doctor talking about mechanism, something I'm very intelligent and smart. Thinking back, that's very stupid. That's very stupid actually. But unfortunately, many of us doctors, scientists, we cannot escape that.
(34:26) the you know brainwash the mechanism of thinking okay we need to break out of the box so first of all for every disease everything we need to really trace back to the true root level drivers whether directly or indirectly okay and but I'm just going to I'm not going to go over this just for your reference here now next because of the time we can discuss a little bit later okay but anyway this I think here this slide this I I put it up in a recent cancer debate hosted by the children's defense, children health defense, you know, that's part of like a think tank
(35:01) to the uh Bobby Kennedy or HH secretary. So I was invited to debate on cancer whether it's a genetic disease or mitochondrial disease. But this is one of the slides I took from there is that you know in the center image as you see here the SMT okay sematic mutation theory the traditional cancer genetic theory the MMT is mitochondrial metabolic theory basically we believe mitochondrial damage is the core of the cancer okay or any broad or many other mechanism the point I'm making here is that these are all mechanisms or the why
(35:38) why the cancer happens. But these theories don't address what causes cancer. Mitochondrial dysfunction didn't cause cancer. Mitochondrial dysfunction is a pathway is a mechanism. All genetic mutations. This actually I want to you know expand a little bit more. Think about it. Even in conventional medicine we believe you know if you look at literature the lit literature says more than 90% of cancers are caused by carcinogens right there's no argument there but why in the clinical medicine and reit focus on mutation mutation is a result is a consequence of carcinogens in the in the conventional medical theory so we need to go to the root cause which is the carinogen as part of it is Right? That's common sense. But today, have you ever heard any oncologist talking about carcinogen? No. Okay. So, this is not just for cancer. But I use this to illustrate.
(36:44) So for me I care more about what are the root drivers that cause either genetic mutations or the mitochondrial dysfunction or other chromosomeal or genetic or any other you know mechanisms that ultimately lead to cancer or other diseases. That's how I think this is what we call root cause analysis. Unfortunately in today's medicine we don't have root cause analysis period.
(37:11) You know everybody, every listener we apply this subconsciously in our problem solving at home at work something happens you want to figure out why right what really caused the problem and unfortunately that important piece is missing in today's medicine okay next so the message of the previous one is that yes we need to understand mechanisms mechanisms you can always argue I tell you as far as there are humans there are people will never end up uh finish arguing there will be always endless okay however root cause levels are only
(37:48) those 10 which I forgot to tell you I already published I mean I uploaded on preprints okay h in my view practically every root level causes will fall into one of those 10 categories okay this is another hallmark okay so we know the last 20 years or so hallmarks medicine becomes very popular the very first one or very first one or two are cancer and aging.
(38:15) Okay, for example, here's hallmarks of aging. I didn't show here due to t constraint of time hallmarks of cancer. But again, these if you look at this, I'm sure you all know about it. It is these hallmarks whether it's aging or cancer they are only talking about what happens in these cancers or aging not what causes for example tieamir attrition genetic mutation like I mentioned mitochondrial dysfunction these are the manifestations okay mechanisms not the root causes we need to go further okay so what I call it the hallmarks medicine that treating patterns not causes Okay, we need root cause medicine. Okay, so basically hormark medicine see the trees and we want to see the forest. Okay, next one. All I list here this is the 10 root drivers I listed here and uh the lower level it's some preprints and here today we're talking about vitamin D as I list here vitam micronutrient deficiencies vitamin D is one of them and you all know I would say at least 80 90% of population worldwide are vitamin D in insufficient or deficient in a way if you don't get enough sunshine you are deficient period. You are English sufficient period. Okay, there's no question about it. This is again vitamin D is a great example I always use is because we all know everybody knows vitamin D is a sunshine vitamin. Okay. And we humans today don't get enough sunshine as we used to after you know highrises and uh western suits fancy clothing we stay inside more than others.
(39:59) So, so if you don't get sunshine, you don't get any vitamin D. Period. There's no questions about it. Next. Okay. So, here is another philosophical uh you know conceptual issues. Okay. We are all used to treat the diseases with so-called guidelines or FDA you know standards. Okay. Well, whereas those are you know do serve their purpose.
(40:25) However, there are you know a lot of issues. Okay, here is my view. We let's go back to hypocratic oath do no harm to patients. Okay, so my view today is that when I apply an you know experimental including higher dose vitamin D the first principle I follow is safety whether what I'm going to do is safe enough.
(40:50) How do I judge whether it's safe or not? Not only the logics physiology but also literature search we need common sense we need physiology biochemistry knowledge okay but also some preliminary study or expert experience for example me I think I am one of the experts and my clinic experience is part of the evidence-based medicine so first of all safety okay guidelines second okay so and with this why is this we know America is a latig ious country you know I prepare always myself whatever I do always prepare can I defend myself in a
(41:27) court of law when I have this in the back burner I never you know knock on the wood saying thank good so far so good okay so first of all safety first then effectiveness okay in terms of effectiveness I al first think about physiology and biochemistry does it serve a physiological biological role if it does it has a place okay then look for clinical evidence and mechanisms do matter here. Okay.
(41:55) Thirdly, affordability and availability and not everybody has access to everything. So when I have those three I recommend to my patients is that simple. So I practically I don't use any other guideline. This is my guideline. I also had it published I mean uh not peer reviewed yet. It's in official u you know pre-print. Okay. Next.
(42:18) So this is my guideline. And so this is my sort of uh blueprint or the sort of uh thinking process or the protocol or what I call it the OM blueprint for health and longevity lifestyle first. I always go in this order free or inexpensive first. Okay? Don't put C in front of the horse. Don't start with fancy expensive stuff.
(42:42) I see that too common in the marketplace. Okay? You lose reputation. You're not serving a patient purpose. All right, it's not so basically don't advise stem cells, IVNAD and these are all fancy marketing gimmicks in my view. So start from cheap free lifestyle. Yes, this is time consuming, energy consuming, but you gain this is their conscience.
(43:07) You make make you feel good and also you gain reputation. You gain more clients. As right now for me, I'm just so busy. I got too many patients. Well, not too many. That was always good. But what I'm saying that the message is you get my message lifestyle first nutritional deficiency as I mentioned vitamin C vitamin D magnesium and other you know critical vitamin minerals very widely insufficient worldwide and deficient.
(43:34) Okay, detox toxins actually now more and more evidence uh toxin overload uh more and more studies begin to show this may be more critical than anything else. Okay, for example, the last 30 years the young the early onset cancer basically patients younger than 50 years of age having cancer the frequency has increased by 80%.
(43:59) Why is that? because of genetic I mean inherit hereditary genetic mutation. No, it's because primarily of the overload of toxins. Okay. So toxin and detox is very critical part. So the first three I believe is the foundation. These actually don't have to cost a lot of money. Okay.
(44:22) I always tell people you go on the on the right side is my recommendation of my diet dietary guideline. Basically, you follow this low fat, low carb diet, low ultrarocessed food and uh you supplement the at least the basic vitamin C, D, magnesium, K2 and omega-3 and detox, exercise, drink a lot of water, stay away from these, you know, over processed food, these things.
(44:48) If you do these three, within a month, one to three months, your health will improve. And these things don't cost you much. In as a matter of fact if you quit these cook these ultrarocessed foods actually may save you money. Now move on further I uh you know mitochondria is the center the core okay and uh you focus on mitochondria nutrition hormonal balance I mentioned about ICV and I you thyroid cortisol and sex hormones and of course biologicals and the regenerative medicine stem cells exosomes peptides all these things but only after you fix
(45:25) the the foundation so in the recent uh I already uploaded onto up uh onto uh uh preprints I intend to publish these academic journals med articles is that anti-aging medicine has two parts the first is to res restore okay upon restoration then you do regeneration okay don't put cut in front of the horse next so so with that uh these are the first few slides I mentioned is basically my conceptual thinking summary of how I view health and medicine and the purpose is for health.
(46:05) Okay, first this is personal. I want to help my parents myself. You know, these are my these are my father and my mother 19 and 88 right now. I'm very healthy. Their house is much better than 10 15 years ago. Okay. And the here is a ultrasound picture here. And we we had a family comprehensive physical exam in Shanghai earlier this year about 10 months, nine months ago.
(46:32) And not surprisingly or surprising to the ultrasound ultrasound doctor our uh the corateed artery is squeaky clean no problems at all for 88 90 and me 66 that's very unusual okay so to me that's not surprising okay that's one number two I want to I should highlight it here my both my parents used to have very high blood pressure their highs can go to like 220 even higher They are low and the diastolic blood pressure often times in the 110 120 very high scary I used to give them like a five I think at one time it was high five uh prescrim drugs but I the
(47:12) blood pressure was hypertension was pretty unstable you know fluctuates a lot that was like 20 some years ago and later on I changed you know as you know I've been learning functional medicine also molecular medicine low car medicine basically I changed their diet I changed their nut nutrition and whatever I've been teaching today.
(47:32) I mean, oh, my parents really believe me. They they take all my advices very religiously and now their blood pressure is very stable. Oh, I'm sorry. This uh this typo here 130 is about 120 some to 130 over 70 to 85 about high. They usually I don't see above 90 now. Okay, pretty stable. Okay, I might add.
(47:56) Okay, so that's a bigger major improvement. And also my mother used to have frequent you know PC u PVCs the ectopic beats of the left ventricle and she can feel the pitation now she doesn't complain anymore and they feel a lot more energetic than before and they live independently they don't I want to hire maids and have they don't want any they live by themselves still but I travel to visit them quite often yeah next for myself I want to be uh healthy this I want first of all let me play A O Jen, can you click on that uh play button? A short video like Yeah. No sound over there. It's all right. Okay. All right. Let me explain a little bit. I love Bington. What I showed you here is that I often when I play Bington I'm kind of all out and I often times I I like to, you know, save every shot uh every shot possible. Okay. Often times I fall down like this.
(49:00) I jump to save these shots and my partners often times they are 20 30 years younger than me you know on bing court how many 60 some year olds you see you don't. Okay. And so often time they will say oh you know Richard or Dr. Ch are you okay? Your bone I jokingly show tell the message I said don't worry my bones may be stronger than you and here on the right is my bone marrow density uh a few years ago as you can see the dot the cross right on on top there and that's my bone density if you draw back to the parallel to the uh on the y this is the y- axis my bone density is probably better than 80 90% of people in their 20th the 30s. Okay, I don't take calcium. Again, here I want to mention, do not take calcium supplements. Okay, I know some vitamin D experts that this is a little bit uh controversial, but my interpretation do not take calcium supplements.
(50:04) If you want to know why, read the Tom Levy's death by calcium. Very convincing, excellent book. Okay. So, I don't take any calcium supplements and uh uh I've been taking all the MM highdose vitamin C, sufficient vitamin D, magnesium, omega-3, and all the other things. Okay. And that's why I can jump on I can fall on floor and no problem.
(50:25) Okay. All right. Next. Oh, I was going to one thing I want to say about this uh endurance. uh one key thing in my view is that I my exercise endurance is much better than most other people uh 20 30 years younger okay and why is that because of this uh because of time let me go a bit faster here I'm going to review a few cases here this is one of the complete reversal yes complete reversal of coronary artery heart disease this patient had up to 69% L left coronary artery narrowing or stenosis in 20 this is I think is a 20
(51:06) months. Yeah, 20 months completely gone. Okay. Just documented by the CTA the angio angography. Next this is another case a complete reversal of coronary artery disease. Again she had a I think 70% coronary stenosis. This is two years exactly actually in uh four years right here and 0% now. Okay. Here I might to I want to add I want to add actually the previous lady not only her coronary artery disease stenosis reversed but also her lung nodules thyroid nodules one disappeared one uh uh improved. Interestingly her aging
(51:51) spot on the cheek faded significantly. What does that mean? because we are targeting the root causes. Chronic diseases can be reversal. Okay. Next. >> We have like one minute so that we can address questions. >> Oh okay. Okay. >> Well this is summarized here but go on. Yeah they can review my slides you can share with them. Yeah.
(52:12) >> Okay. >> Go on next. >> Yeah. Well this is varicose vein also you know improved. Go on next. cancer actually with the same approach metabolic this patient is now seven years eight years now cancer free next okay so basically I didn't show you because of time we also with this same approach we we improved diseases yes Hashimoto's lupus osteoporosis is irreversible we have couple se several cases of osteoporosis being cured by bone marrow I mean measured by bone marrow density. Okay.
(52:55) And next, well, this is actually to join me at this 21st century medicine because I'm summarizing these things in a book and you we can read here. All right. Any questions? Yeah. >> Oh, yes. We've got a lot of questions. >> Okay. >> So, I'm going to stop sharing the screen right now. I saw a few questions came in um while you were doing your review, but I'm going to just go ahead and read through some of the questions that were submitted ahead of time.
(53:24) And I know you addressed uh some of them already. Um but first I'm going to say um this is from Dr. Nazir Edin Kabir, a PhD in nutrition um in Algeria. And he says, "In recent years, we observe a growing number of individuals with adequate or even high serum 25 hydroxy vitamin D levels who nevertheless exhibit functional signs of vitamin D insufficiency.
(53:53) From your clinical and medic and mechanistic perspective, how do you interpret the concept of vitamin D resistance? And what role do factors such such as magnesium deficiency, chronic inflammation, obesity, genetic polymorphisms of the vitamin D receptor and impaired impaired hydroxilation play in this phenomenon? And I know you addressed some of that, but if you have additional comments, that would be great.
(54:21) uh practically we already covered all those and like I mentioned uh multiple factors for example specifically you magnes I mean vitamin D magnesium vitamin K2 are sort of tied together and uh we know one we mentioned about a little bit earlier magnesium and calcium are antagonists to each other so we should never discuss calcium without discussing vitamin I mean magnesium and we know vitamin K2 is also sort of uh you know soft tissue calcium uh deposit uh uh antagonist so to speak so you know so that's a very important part that I use in my protocol for example
(55:01) personally I take 45 milligram yes 45 migram of vitamin K2 daily why because that's the minimum in at least one study minimum uh concentration or level showing that uh it pas itself is able to reverse osteoporosis >> and it's expensive but I can afford it so so I want to take it you know. Yeah, there was a question that actually came in while you were talking on the same topic um about vitamin A which is necessary to modulate vitamin D function and he says uh it's a common partner the active form of vitamin D or calcatrial must form a complex with the retinol retinoid X receptor a vitamin A receptor to activate target genes. If high levels of vitamin A are present, its metabolites can dominate or you utilize much of the available RXR proteins, leaving fewer available to partner with the vitamin D receptor. This competition for the common RXR partner can compromise vitamin D's ability to carry out its functions, such as regulating calcium metabolism.
(56:11) And he argues it is hormones from the serum to the cytoplasm that are upstream, cortisol and insulin are downstream. Do you have any uh any comments about that? >> Yes, actually that's an excellent question. The question is again like I mentioned you know in today's medicine we sort of uh you know look at the holistic you know uh look at an individual only look at one part when we talk about vitamin D we only talk about vitamin D and not vitamin A.
(56:38) Well, let me tell you, I already mentioned a little bit about vitamin C and you know ICV excess I mentioned a little bit but you can talk a lot practically. We have to remember our body is very intricate. God or mother nature designed our body to be very complex. It's beyond our comprehension. So how do we deal with such a complex system? My view is that uh first of all we admit there are so many other factors working together as a teamwork.
(57:11) Okay, that's number one. Number two, so individually I try to study all these vitamin A, C, magnesium, D you know uh you know to see what is their safe level and optimal range. Okay. And then I try to uh manage these levels to right now I'm trying to aim for the you know midpoint of the normal range within these for example vitamin A included yes he the the that the commentator was absolutely right the view how do we I mean you know like I mentioned there are so many other factors so basically what I'm view right now is that regardless how these
(57:54) mechanisms work how these toxins work the my view is that if it's toxic if it's a foreign thing to our body try to use as little as possible okay ultrarocessed foods are not natural try to minimize I'm not saying it's it's impossible to completely get rid from our life but minimize intentionally at least okay so basically what our body doesn't need normally is not part of body try to be be very cautious when using it I try to stay away from those things our body normally it's part you know you know whether it's a mineral or vitamin it's normal part of physiology biochemistry try to see what is the best you know optimal level and achieve that in my view regardless the chaotic mechanism in between we everybody can talk 10 days or you know on these things but every nobody will agree on any why because the my view is that I don't care how it is let's do this and you know what clinically as I personally experienced many health conditions disease improve.
(58:58) >> Right? >> That's the answer. Yeah. >> Thank you. And I do see a couple questions about specific slides and a couple comments and and I just want to say I'll send these to you separately, Dr. Chang, so that I can communicate the answers with the uh individuals asking and you can always follow up uh those who are watching with me, Jen, at grassrootsalth.
(59:19) org uh if you still have questions that we don't get to. Um I wanted to mention another question. Um, so for years I've read Grassroots Health from the beginning, I believe. Uh, so I've long been encouraging people and patients, I'm a nurse, to work hard to get their vitamin D levels uh to at least 50 and if possible even higher.
(59:41) But now I'm getting some push back about vitamin D supplementation might interfere with melatonin production and thus impair sleep. How do I answer this? I would like to hear more about the inter interaction between melatonin and vitamin D. I read your paper and it does address it nicely but it would be interesting to discuss it and expand upon it.
(1:00:00) >> Yes, that's a very interesting question to we still we again should think to be back you know put these things into back off physiology. Vitamin D we know it is actually a sunrising hormone right it's a daylight hormone it's a regulator of our circadian rhythm so when we you know naturally uh when we during daytime we get out we get sunshine vitamin D level goes up and it yes it can uh you know helps regulating the melatonin it does it does indirectly probably and so some people uh may experience if you take
(1:00:37) vitamin D at night it may have a little bit awakening effect possibly but actually more predominantly for those people who are deficient in vitamin D vitamin D help their sleep >> that's more common yeah in a window these are like sort of bifphasic you when you're low you know when you define vitamin C the same vitamin C actually calms your brain calms your adrenal cordex but it also because gives you more energy some people report they feel a bit energetic so if that's the case for we take it in the morning like the sunrise take it in the morning right so that's very interesting I talking about here actually I want to add a little bit more melatonin interesting melatonin we have two sort of you know we have the pioneer pioneer gland secretive melatonin which plays more into our circadian rhythm but we also have a lot of melatonin in our mitochondria which is locally produced and locally effective antioxidant so those are a little bit different yes anyway in summary vitamin V does affect vet vitamin D but that's not the reason not to okay we mentioned that 50 great that nurse is doing great job helping our patients and that's okay to be 50 if you want to push higher to 80 that's fine 100 that's fine too >> yeah so I think you also addressed a question that just came in what influence does vitamin D have on sleep and I've also seen the studies that correcting deficiency can improve sleep >> um and so I'm going to Mark that is done and then okay I have another question um and I I I would like to hear your view on this because and okay for someone
(1:02:18) with accidental overdose of vitamin D for a few weeks reaching a level of 160 nanogs per milliliter which I'll pause there because I I wanted to know how did they know that they overdosed or they just accidentally took more than they wanted because I wouldn't see 160 as being toxic yet as you addressed in your presentation, but I'll continue on with the question.
(1:02:42) Is it advisable to take high doses of magnesium and K2? Because there was a study from Grassroots Health that participants taking both increase their vitamin D levels substantially while taking the same amount of vitamin D. I'm worried that by taking more magnesium and K2, the vitamin D levels will ride rise higher. >> Well, again, yeah, we already mentioned this.
(1:03:05) you know I never take or I never advise any particular nutrient supplement alone. This is my holistic view you know and talking about magnesium and uh K2 those are very critical question like I mentioned ASCVD is the number one killer the top killer for developed areas nations and so personally this is one of our most interested areas and as we we should know whether hypertension or SCVD calcium dep deposition into into blood vessel is a critical issue here.
(1:03:42) Okay, how do we do that? How do we counter that? Is first of all, don't take calcium supplements. Period. We got a plenty of calcium in our foods. Okay, those people who think uh we our food is lack of calcium, people don't have enough calcium, most likely because of vitamin D deficiency, they don't absorb enough. Okay, because we know vitamin D insufficiency is at least 80% maybe more I think more.
(1:04:06) But anyway, so that's first. Number two is that is that we want you know we want calc magnesium to calcium is a is a exciting agent in intracellular exciting agent. They basically they increase your cellular excitability. They make your cells spasmatic. Okay. So that's why you have leg cramps, you have headaches, you have tension that contributes to that and also ectopic beats.
(1:04:35) Magnesium antagonizes that. So magnesium relaxes cells. Okay, we need today we are most people are magnesium insufficient and calcium too much. Okay, now potassium I mean K2 K2 is critical is because now we know not only middleage to older people having you know uh calcium basically calcium deposits in our soft tissues, lungs, thyroids and breasts, prostates but also blood vessels more more critically.
(1:05:06) young people even younger than you know toddlers they they've been reporting this okay so I I say K2 should be a you know if you can afford take as much as you can not just 100 microgram 200 microgram that's the minimum like I said I myself take 45 milligram at least for those people middle age I recommend 1,000 microgram or one milligram I recommend magnesium at least you know the elemental magnesium maybe around 500ish, you know, magnesium glycinate maybe 2,000ish milligram a day, you know, I'm go because these things are very safe. My again safety first. Matt
(1:05:44) is magnesium is very safe by by mouyj. The worst case scenario, diarrhea. Okay. Yeah. >> Okay. And I do want to comment our very last vitamin D study hour was on that topic of the calcium to magnesium ratio with Dr. Silwansa. So, there's a lot more information on that topic uh posted to our YouTube right now.
(1:06:08) Um, and I'm I'm going to end with just a couple of questions kind of combined and then I'll follow up with a comment. Um, but uh I do have somebody who asked who's a nurse, do you recommend a reputable orthomolelecular program for nurses? And then I also had somebody write in um and she asked which specialty doctor would be best to work with to get optimal vitamin D and mineral levels and she specifically pointed out the imbalance of calcium and magnesium.
(1:06:41) That's a very excellent question and uh as Jay mentioned I'm the editor and chief of also medical medicine news service which uh developing these training courses is one of my strong interests but you know this is a teamwork and I think Jen maybe two three years ago when we had our first you know global conference we mentioned that I would need a lot of organizational help because you know I'm a I think I am more of a of a physician scientist type of person rather than organize. I'm not but I like too. Yeah.
(1:07:13) But I I also molecular medicine news service we publish these regularly and uh as you may have noticed actually I'm about to write an article editorial on that magazine telling the readers how what I'm thinking how basically like today I'm talking about conceptual issues first then we get deli dive deeper into each you know detail things because I get questions from patient readers want to detail the discussions. Yes, I know we need that.
(1:07:44) But don't forget the big picture. I like to see the big picture first. All right. So, yes. And uh in terms of vitamin D and magnesium or these things, this actually I would my advice is looking for an experienced author molecular medicine particularly from grassroots health you know Dr. J I mean Jen's group and also Jen is by the way she is on our editorial board at also miracle medicine news service. Okay. So we work together and also at our most also because the these are the kind of people our author nutrition is more than conventional nutrition is goes much into deeper into mechanisms orings and outs than functional medicine or any other fields >> right yes so uh again email me my email jenjengrassealth.
(1:08:38) org if you have questions or want specific referrals um because we do work together. We've got a great network and I can always refer out as well. Um I'm going to end with a uh comments. Uh Dr. Chang, I read your article on understanding and addressing vitamin D resistance with great interest and attention.
(1:09:00) The entire analysis is excellent. I believe that resistance only occurs when there is an inadequate vitamin D level but a lack of action at the receptor. Other times it is a deficiency which is not the same as resistance. Undoubtedly patients with cancer or autoimmune diseases should have much higher levels than 40 or 60 or even 80 to 100.
(1:09:21) Um do you have any comments on this and we'll end with this one. We I like to see you know if we can having organized you know because I'm an individual but if we can group together do studies like I mentioned I think you mentioned I like to see what is really the optimal range for anti-aging and like I mentioned anti-aging should have two parts the first is the reversal prevention of chronic diseases if you don't die of cancer if you don't die of heart disease then we can talk about anti-aging so so first of all what be the what will be the optimal range The second is can we start designing or or thinking at least of studies to to push towards that direction. That is very interesting area. >> Yeah. And I would be curious you know because Dr. Cobra himself uh he determines the optimal dose based on the PTH level uh not the vitamin D level. And so it would be really interesting to add those types of measurements to a study so that we can see the variability in what somebody's optimal dose needed for overcoming that vitamin D resistance could be based on looking at PTH and other markers. >> May I add something? >> Definitely. >> Yeah. I think you know out of all these you know we're talking about root causes today and uh talking about the regulatory mechanisms a few I think are more critical for example oxidative stress inflammation mitochondrial function and today we just added the hormonal regulation the ICV into the BHRT axis.
(1:10:56) I think uh when we determine the ultimate uh uh the outcome we should address these or at least include as many as possible you know in our study in our thinking not just one >> right 100% agree and with that um I want to thank you again Dr. for joining us and covering this very interesting topic. Do you have any last uh comments, questions, anything you want to close with? >> Oh, okay.
(1:11:29) I think this is a great field and those who came to our conference obviously realizes the deficits in the conventional medicine and we should push forward towards patient oriented health care and so let's if possible let's join together and let's promote true health. I'm not against making money but patient care first, health care first, money making second.
(1:11:53) >> Thank you. All right. Well, thank you again everybody for joining us today. I'm looking forward to seeing you again after the holidays. Happy holidays. Happy holiday. Hopefully you join us on uh January 7th with Dr. Michael Hollik. Right. Have a great day. >> Bye-bye everybody. >> Thank you again."