Vitamin D tests: current and future (no blood spot, no Y/N) - June 2026
How vitamin D is measured in your blood — and what's coming next
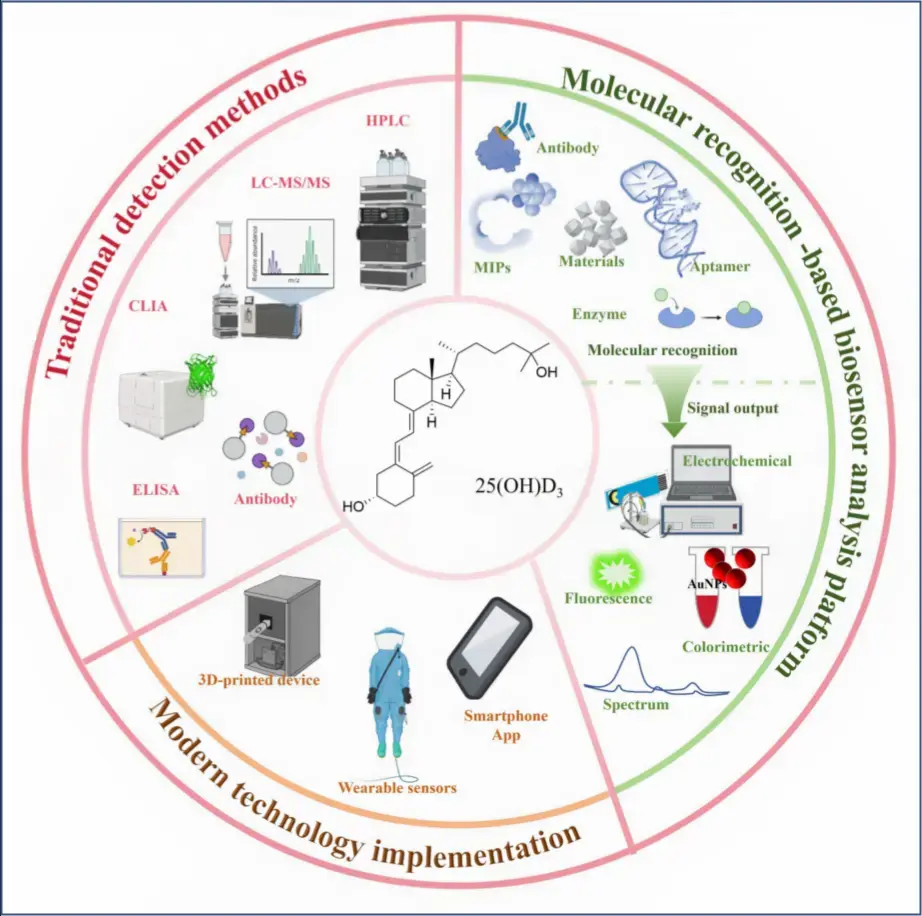
A plain-language summary of a June 2026 review of vitamin D testing technology. Source: Bi D, Cheng Y, Sun X, Xu Y. "A Comprehensive Review of Analysis Strategies for 25-Hydroxyvitamin D3: Mechanisms, Platforms, and Future Perspectives." Biosensors 2026, 16, 314. https://doi.org/10.3390/bios16060314
Dehui Bi, Yiran Cheng, Xinyang Sun and Yuancong Xu CHINA
The 30-second version
- When a lab measures your "vitamin D level," it is almost always measuring 25(OH)D3 (25-hydroxyvitamin D3) — the main form circulating in your blood and the best marker of your overall vitamin D status.
- Today's tests fall into two families: big-instrument lab methods (very accurate, slow, expensive) and immunoassays (fast, cheaper, but less consistent between labs).
- A large wave of experimental "biosensor" tests is in development — small, fast, and potentially usable at home or in a clinic. Some are extraordinarily sensitive on paper.
- The honest caveat: nearly all of these new devices are still in the laboratory. They are not yet things you can buy. And all of them, old and new, still rely on a blood sample.
Why the test is called "25(OH)D3" and not just "vitamin D"
Vitamin D goes through several steps in the body. Sunlight or supplements give you vitamin D3. Your liver converts that into 25(OH)D3, which builds up in the blood and lasts for weeks. Your kidneys then make small amounts of the active hormone, 1,25(OH)2D3, as needed.
Because 25(OH)D3 is stable and reflects your long-term supply, it is the form labs measure. The review uses these common cut points (in nanomoles per liter):
| Status | 25(OH)D3 level |
|---|---|
| Deficient | below 50 nM (about 20 ng/mL) |
| Insufficient | 50–75 nM (about 20–30 ng/mL) |
| Sufficient | 75 nM and above (about 30 ng/mL and above) |
Note: these thresholds are the ones cited in this particular review. Where the line should be drawn is itself an area of active scientific debate, and different expert groups set it differently.
The tests used today
Big-instrument lab methods (the "gold standard")
LC-MS/MS (liquid chromatography–tandem mass spectrometry) is treated by the review as the most accurate method available. Its key strength: it can tell apart closely related molecules — D2 from D3, and a look-alike called 3-epi-25(OH)D3 that can fool simpler tests.
- Strengths: Extremely accurate and sensitive.
- Limitations: The machine can cost more than $100,000; samples need extensive preparation (more than half the total testing time); throughput is limited; and it requires trained specialists. This is lab-only technology.
HPLC (high-performance liquid chromatography) is an older instrument method — accurate, but needs large samples and skilled operators.
Immunoassays (what many clinical labs actually run)
These use antibodies that grab onto 25(OH)D3. Most automated hospital analyzers (made by Abbott, DiaSorin, Roche, Siemens and others) work this way.
- Strengths: Fast, automated, lower cost, high throughput.
- Limitations the review flags directly:
- Lab-to-lab disagreement. Results from these assays don't always match LC-MS/MS, and standardization between methods is an unsolved problem. This is why the same blood can give somewhat different numbers at different labs.
- Cross-reactivity. The antibodies can mistake 25(OH)D2 for 25(OH)D3, which can push a result falsely high.
An older version, RIA (radioimmunoassay), is now largely replaced because it produces radioactive waste.
The new wave: biosensors
Most of the review covers biosensors — small devices that turn "vitamin D is present" into a measurable signal (a color change, a glow, or an electrical current). Researchers are trying many designs. A few highlights, in plain terms:
- Aptamer-based sensors use a short piece of synthetic DNA (instead of an antibody) as the "lock" that 25(OH)D3 fits into. Aptamers are cheaper, more stable, and longer-lived than antibodies — they can survive heat and storage and be reused. The most-studied one is called VDBA14.
- Electrochemical sensors measure a tiny electrical change when vitamin D binds. With signal-boosting tricks, some reach astonishingly low detection limits on paper.
- Optical sensors read a color or light change — including very sensitive lab techniques (SERS, SPR) and simple lateral flow strips much like a pregnancy or COVID test.
- Smartphone-read strips. Several prototypes pair a test strip with a phone camera and an app to read the result — one used only a fingertip drop of blood and gave a result in about 15 minutes.
- Wearables. Early prototypes include a sensor built into a mouthguard and flexible chips meant for continuous monitoring.
How they compare (from the review)
| Approach | Speed | Cost | Where it works |
|---|---|---|---|
| LC-MS/MS (gold standard) | 30–60 min/sample | Very high (>$100k machine) | Reference lab only |
| Immunoassay (CLIA/ELISA) | Moderate | Moderate | Hospital/clinical lab |
| Biosensor (experimental) | ~5–15 min | Potentially low | Clinic, point-of-care, possibly home |
What this technology does NOT do (yet)
In keeping with an honest reading of the evidence:
- It is not available to buy. The review states plainly that nearly all of these biosensors remain at the laboratory-research stage. The very low "detection limits" you may see quoted are lab measurements under ideal conditions, not proven real-world accuracy.
- It does not remove the need for a blood sample. Even the portable devices still rely on blood (often a fingertip drop). The review names truly non-invasive sampling (saliva, for example) as a goal that has not yet been achieved.
- One whole sensor category is limited. Sensors built from "molecularly imprinted polymers" (MIPs) are durable but, by the review's own account, far less sensitive than the antibody and aptamer types.
- Some designs can't tell vitamin D forms apart. For example, one enzyme-based sensor could not distinguish 25(OH)D3 from the active hormone 1,25(OH)2D3 without redesign — the same kind of specificity problem that affects standard antibody tests.
The practical takeaway for readers
- If you get a vitamin D test today, it is measuring 25(OH)D3, and it is almost certainly either an LC-MS/MS lab test or an automated antibody immunoassay.
- If you compare results from two different labs and they don't match, that is a known and documented issue, not necessarily an error in either test. Try to track your levels using the same lab and method over time.
- Cheap, fast, at-home vitamin D testing is being actively developed and the engineering is promising — but it is not here yet, and the headline sensitivity figures are laboratory results, not consumer-product performance.
By Claude AI - June 2026
Related in VitaminDWiki
- Tests for Vitamin D
- Vitamin D test result can vary by 40 ng (10 reasons)
- Find out if you might be vitamin D deficient for free - 2 minutes, 11 questions
- How to compare Vitamin D measurements from multiple studies
- 4 popular vitamin D testers gave very different results (no surprise)
- Vitamin D testing accuracies, including dried blood spot
- Low-cost Vitamin D testers (two yes-no tests for 11 dollars) - 2024
- Vitamin D deficiency of a group - 15 pcnt to 48 pcnt (depends on tester used)
- 50,000 IU monthly safe to take without any vitamin D testing – RCT