Poor health often associated with low Vitamin D - Review Feb 2026
Vitamin D deficiency and disease conditions relevant to: Orthopaedic translation
Review J Orthop Translat. 2026 Feb 22:57:101061. doi: 10.1016/j.jot.2026.101061
Dinayinie Ekanayake Mudiyanselage 1, Charles Edward Ouyang 1, Rebekah Ding Jin 1, SriHarshidha Velmurugan 1, Yunze Jiang 1, Jiashi Sun 1, Daqing Ma 1 2 3
Vitamin D, traditionally known for its role in calcium-phosphate homeostasis and bone health, is now recognised as a pleiotropic hormone with critical effects on multiple physiological processes. It exists primarily as ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3), which are biologically inactive until undergoing a sequential hydroxylation in the liver to form 25-hydroxyvitamin D (calcidiol), and subsequently in kidney to form the active metabolite 1,25-dihydroxyvitamin D (calcitriol). By engaging the vitamin D receptor, it exerts immunomodulatory, neuroprotective, and anti-frailty functions.
Deficiency in vitamin D has been implicated in a wide range of disorders, including musculoskeletal weakness, frailty, cognitive decline, autoimmune diseases, and respiratory infections. Vitamin D deficiency affects nearly half of the global population and remains a widespread public health challenge, and effective interventions such as food fortification and targeted supplementation should be prioritized in future strategies.
The translational potential of this article: Vitamin D deficiency represents a modifiable risk factor with implicated effects across systemic, neurocognitive and musculoskeletal systems. Epidemiological evidence links deficiency to increased risk of infection, cognitive decline, frailty and orthopaedic morbidity. In orthopaedic and geriatric populations, maintaining sufficient vitamin D supplementation may reduce fracture and fall risk as well as postoperative complications and infections. These factors are also influenced by vitamin D deficiency-related effects on neurocognition. Vitamin D status may also be relevant in the management of infectious diseases, including respiratory illnesses and COVID-19. This review also discusses mechanistic and practical rationales for clinical translation. Potential interventions include vitamin D co-supplementation, dietary fortification and optimised sun exposure. However, limitations in existing randomised trials underscore the need for consistency in dosing, appropriate formulation, targeted population, as well as baseline deficiency progression status. These insights can guide clinicians, public health policy makers and researchers in developing evidence-based protocols and interventions to reduce vitamin D deficiency-related morbidity.
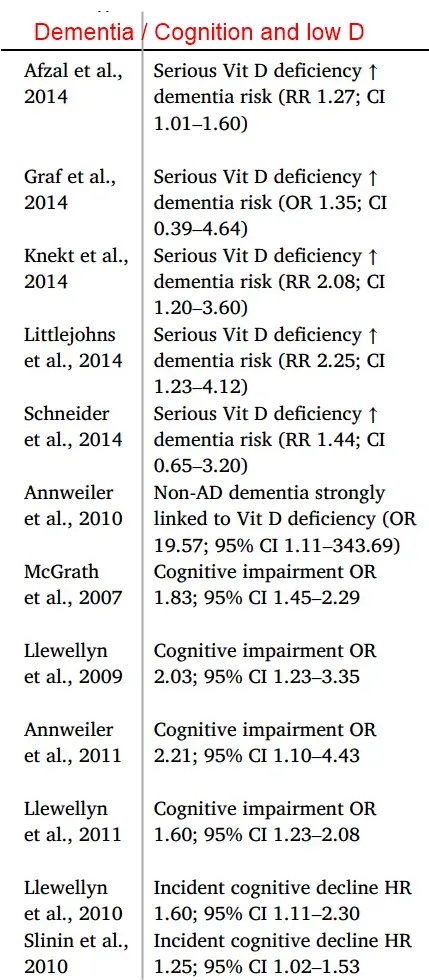
Cognition / Dementia and Vitamin D
Conclusion (From the PDF)
Vitamin D deficiency is a significant public health concern linked to frailty, cognitive impairment and increased risk of infection, fractures and falls, particularly among the ageing population. As such, its role extends beyond calcium and bone metabolism to include regulation of immune response, neuroprotection and bone-muscle function.
Vitamin D plays a crucial role in innate and adaptive immunity. Through promoting antimicrobial peptide production, supporting tolerogenic dendritic cells, and regulating T-cells, Vitamin D modulates inflammation and immune tolerance [33,35,36]. Vitamin D deficiency has been linked to heightened pro-inflammatory states [199], impaired pathogen clearance [46], and increased risk of autoimmunedisease [36], highlighting its importance for immune health. Lower preoperative vitamin D levels are repeatedly reported with higher postoperative infection risk, likely due to reduced LL-37-mediated antimicrobial activity and impaired biofilm control at implant surfaces [39,41]. Host defence may also be compromised due to an acute postoperative decline in vitamin D status during inflammatory stress [42]. These highlight the orthopaedic translation of sufficient vitamin D in infection prevention and inflammation control and determine postoperative outcomes.
Beyond immunomodulation, Vitamin D deficiency is associated with impaired cognition [69], language development [75,76] and increased risk of neurodegenerative and psychiatric disorders [20,164,245-249]. As such, evidence demonstrates that Vitamin D influences neuronal growth, synaptic plasticity [59], neurotransmitter regulation [60] and neuroprotection [172]. Evidence from both human and animal studies links Vitamin D deficiency to altered brain morphology [52-55],dopaminergic system development [60] and increased risk of dementia [164] and Alzheimer’s disease [20,245]. However, randomised trials yield mixed results, underscoring the need for high-quality, standardised clinical studies to validate the therapeutic potential of Vitamin D.
Vitamin D deficiency is highly prevalent in older adults and contributes to key components of frailty, such as sarcopenia and increased risk of fractures. Vitamin D/VDR signalling regulates muscle proteo- stasis, calcium handling, and myogenesis [106], while supporting bone mineralisation through calcium absorption and osteoblast activity [118]. Vitamin D deficiency leads to increased muscle protein degradation and inflammation. Although animal models robustly support these mechanisms, human studies show inconsistent results, likely due to variability in Vitamin D status, dosing and population differences. These factors may also explain the context-dependent results seen in clinical studies that highlight the role of vitamin D in influencing falls, fractures and functional capacity. Maintaining sufficient daily vitamin D intake appears more clinically beneficial than high intermittent dosing, reinforcing its relevance in frailty management, musculoskeletal health and orthopaedic care [136,250,251]. Vitamin D deficiency is also linked to increased susceptibility and severity of infectious diseases, particularly respiratory tract infections such as tuberculosis [195] and COVID-19 [199]. Vitamin D induces antimicrobial peptides like cathelicidin and defensin and mitigates excessive inflammation by suppressing IL-6 and TNF-a, proinflammatory cytokines [8,187-190]. Although meta-analyses have found reduced acute respiratory infection risk with vitamin D supplementation, translation of these effects is limited. These may be attributed with inconsistencies among intervention trials highlighting the need for further validation before clinical recommendations for Vitamin D supplementation can be made.
Vitamin D deficiency is common in orthopaedic patients and has important implications for fracture healing, neuromuscular function, and postoperative recovery [210-212]. While epidemiological studies consistently associate low serum 25(OH)D levels with adverse musculoskeletal outcomes, large, randomized trials in largely vitamin-D-replete populations show limited benefit from routine supplementation [214,215]. These findings underscore the importance of a targeted, test-and-treat approach in orthopaedic practice, with selective testing at key clinical decision points and individualized repletion for patients with documented deficiency [208,220]. Diet, food fortification, and sun exposure contribute to baseline vitamin D status but are insufficient to achieve timely correction in high-risk orthopaedic populations and should, therefore, be regarded as supportive public-health measures rather than definitive therapeutic strategies.