Phosphate food additives quietly lower your active Vitamin D
Phosphate food additives quietly lower your active Vitamin D (via FGF23 → CYP24A1)
Summary. Inorganic phosphate additives — among the most consumed substances in the modern processed-food supply — are absorbed far more completely than the phosphate naturally bound in whole foods. That hidden phosphate load raises the hormone FGF23, and FGF23 in turn suppresses CYP27B1 (which makes active vitamin D) and induces CYP24A1 (which destroys it). The net effect is lower circulating 1,25(OH)2D (calcitriol) plus an independently cardiotoxic rise in FGF23. This page argues that phosphate additives are a distinct, under-recognized drain on the active vitamin D pool — and explains why, on this pathway, the fix is cutting the additive, not simply taking more vitamin D.
Companion page: "Some food preservatives increase hypertension by ~30% (Vitamin D might reduce the %)." That page covers the renin/RAAS arm, where good vitamin D status is plausibly protective. This page covers the phosphate arm, which behaves differently and is the more direct vitamin D story.
Key points
- Phosphate from additives is ~80–100% absorbed; phosphate naturally bound in food is only ~40–60% absorbed. The additive form is the "hidden," highly bioavailable load.
- A phosphate challenge raises FGF23, even in healthy people with normal kidneys.
- FGF23 lowers active vitamin D two ways at once: it suppresses CYP27B1 (less calcitriol made) and induces CYP24A1 (more calcitriol broken down).
- Elevated FGF23 is independently linked to cardiovascular harm — left ventricular hypertrophy, vascular calcification, and CVD events/mortality — in CKD and general-population cohorts.
- The asymmetry that matters: on the phosphate pathway, vitamin D is not cleanly protective. Calcitriol itself raises phosphate absorption and also induces CYP24A1, so "take more D" does not neatly offset phosphate-additive harm. The clean lever is reducing inorganic phosphate additives.
- Intervention evidence: in community-living adults, lowering phosphate-additive intake reduced FGF23 — a modifiable, real-world target.
- Phosphate intake is badly underestimated because additive phosphate is largely unlabeled (listed only as "phosphate," "phosphoric acid," or E338/E450–E452, with no quantity).
Why additive phosphate is different from food phosphate
Phosphorus in whole foods is mostly organic — bound to proteins, lipids, and phytate — and must be enzymatically hydrolyzed before absorption, so only a fraction gets in. Inorganic phosphate added during manufacturing is already free, highly water-soluble, and absorbed almost completely. Absorption estimates for additive phosphate run roughly 80% to nearly 100%, versus about 40–60% (and far less for phytate-rich plant sources) for natural food phosphorus. The practical consequence: total phosphorus intake badly underestimates the absorbed load, because the source matters as much as the amount.
This is why phosphate additives are sometimes called a "hidden" exposure. They appear on labels only as vague terms — phosphoric acid (E338), di-/tri-/polyphosphates (E450–E452), and related salts — with no quantity disclosed, even though di-, tri- and polyphosphates reached roughly 70% of participants in the NutriNet-Santé cohort.
The hormonal cascade: phosphate load → FGF23 → less active vitamin D
The body defends against a rising phosphate load through FGF23, a phosphaturic hormone secreted by osteocytes. A high phosphate intake — and additive phosphate in particular, because it spikes serum phosphate quickly — drives FGF23 up.
FGF23 then does two things to the vitamin D system at the kidney, in the same direction:
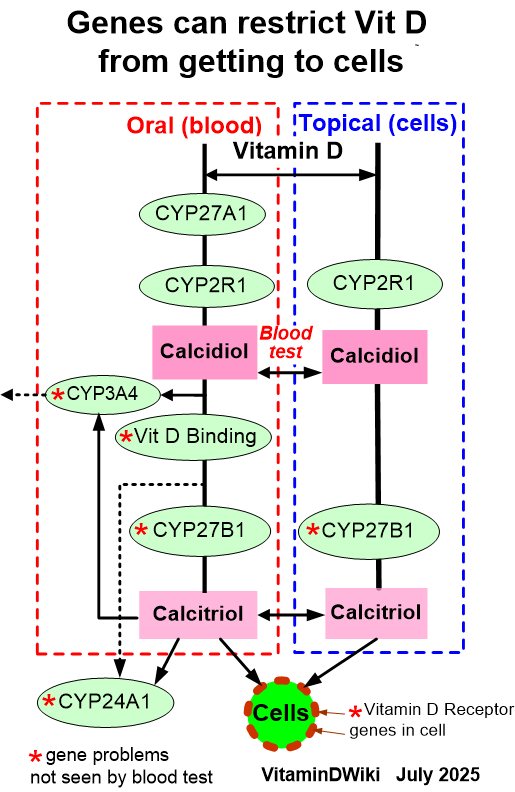
- Suppresses CYP27B1 (1α-hydroxylase) — the enzyme that converts storage 25(OH)D into active 1,25(OH)2D. Less active vitamin D is produced.
- Induces CYP24A1 (24-hydroxylase) — the enzyme that inactivates 1,25(OH)2D (and 25(OH)D) down the C-24 oxidation pathway. More active vitamin D is destroyed.
So FGF23 throttles synthesis and accelerates catabolism simultaneously, pulling circulating calcitriol down from both ends. (This is the mirror image of PTH, which stimulates CYP27B1 and suppresses CYP24A1.) Note the closed loop: active vitamin D itself also induces FGF23 and CYP24A1, which is exactly why the phosphate arm is not a simple "more D fixes it" story — see the asymmetry section below.
The CYP24A1 induction step is the same control point implicated in the broader "why does supplemental vitamin D sometimes underperform" question, and the same enzyme targeted by CYP24A1 inhibitors (e.g., the curcumin work). A chronically high phosphate-additive intake can be understood as a standing signal that keeps CYP24A1 leaning toward catabolism.
Why elevated FGF23 is itself harmful
The FGF23 rise is not just a vitamin D problem — FGF23 appears to be directly cardiotoxic:
- Left ventricular hypertrophy (LVH). FGF23 can induce LVH directly in cardiomyocytes, through a signaling route that does not require its usual co-receptor Klotho.
- Vascular calcification and arterial stiffening, tied to the broader phosphate-load picture.
- CVD events and mortality. Higher FGF23 and higher serum phosphate track with cardiovascular events and all-cause mortality across chronic kidney disease cohorts and in the general population — even at phosphate levels still inside the "normal" range, after adjusting for kidney function and BMI.
This gives phosphate additives a plausible double hit: they erode the active vitamin D pool and, through the same FGF23 elevation, push cardiovascular risk independently.
The asymmetry: why "just take more vitamin D" does not fix the phosphate arm
This is the most important nuance, and the reason this page is a separate story from the renin/hypertension page:
- Calcitriol increases intestinal phosphate absorption (it up-regulates the NaPi-IIb transporter). So high vitamin D activity adds to phosphate load rather than relieving it.
- Active vitamin D induces CYP24A1 and FGF23 as part of its own feedback loop — the very steps that lower active vitamin D and raise cardiovascular-relevant FGF23.
In other words, the phosphate–FGF23–vitamin D system is a bidirectional loop, not a one-way street where more vitamin D buffers the damage. On this pathway the harm and the response are entangled, so the honest, defensible position is:
Phosphate additives degrade the active vitamin D pathway (via FGF23 → CYP27B1↓ / CYP24A1↑) and raise an independently cardiotoxic hormone. The clean intervention is reducing inorganic phosphate-additive intake, not increasing vitamin D. More vitamin D is not established as a counter-measure here and could, in principle, add to phosphate absorption.
This is deliberately not symmetric with the companion page's renin hypothesis (where good vitamin D status plausibly helps). Keeping the two arms distinct protects the argument's credibility.
The good news: this is modifiable
Unlike many exposures, phosphate-additive load is highly actionable:
- Lowering phosphate-additive intake reduces FGF23 in community-living adults — demonstrated in interventional work, not just observed in cohorts.
- Restricting inorganic phosphate additives lowers serum phosphate in kidney-disease populations, and plant-forward eating patterns tend to lower FGF23.
- Because additive phosphate is the highly bioavailable fraction, avoiding processed foods with phosphate additives removes a disproportionate share of the absorbed load for a relatively small change in food choices.
Where this connects on VitaminDWiki
- CYP24A1 control point. Phosphate additives are a dietary lever on CYP24A1 induction — relevant to the curcumin/CYP24A1 thread and to the general question of why active vitamin D can run low despite adequate 25(OH)D.
- Ultra-processed food (UPF). Phosphate additives are one concrete, mechanistic reason UPF diets may harm cardiovascular and bone health, beyond calories and sodium.
- Companion hypertension page. Together the two pages make the point that "preservatives" is not one mechanism: the renin/sodium arm and the phosphate/FGF23 arm interact with vitamin D in opposite ways.
Research gaps to flag
- No large cohort has yet, to our knowledge, tied measured additive-phosphate intake to serum 1,25(OH)2D and CYP24A1 activity in the general population — the direct test of the "additives lower active vitamin D" claim.
- The relative contribution of additive phosphate (vs. total phosphorus) to FGF23 elevation in healthy, normal-kidney adults needs firmer quantification.
- Whether reducing phosphate additives measurably raises active 1,25(OH)2D (not just lowers FGF23) is an open, testable question.
Bottom line
Phosphate food additives are a high-prevalence, highly bioavailable, largely unlabeled exposure that raises FGF23 — which simultaneously suppresses production (CYP27B1) and accelerates catabolism (CYP24A1) of active vitamin D, while independently elevating cardiovascular risk. The right response on this pathway is to limit inorganic phosphate additives, recognizing that — unlike the renin/hypertension arm — more vitamin D is not a clean fix and may even add to phosphate load.
References
Phosphate-additive bioavailability and the UPF link
- Calvo MS, Uribarri J. Public health impact of dietary phosphorus excess on bone and cardiovascular health in the general population. Am J Clin Nutr. 2013;98(1):6-15.
- Erem S, Razzaque MS, et al. Industrial use of phosphate food additives: a mechanism linking ultra-processed food intake to cardiorenal disease risk? (review). PMC10459924.
- Phosphate-based additives in processed foods: is excess exposure a cause for concern? A cross-sectional examination of the United States packaged food supply. Am J Clin Nutr. 2025.
FGF23 and vitamin D metabolism (CYP27B1↓ / CYP24A1↑)
- Shimada T, Hasegawa H, Yamazaki Y, et al. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004;19(3):429-435.
- FGF23 and vitamin D metabolism (review). PMC8674776.
- Bikle DD, et al. Vitamin D: metabolism, molecular mechanism of action, and pleiotropic effects. Physiol Rev. 2016 (FGF23/Klotho suppress CYP27B1, induce CYP24A1).
FGF23 and cardiovascular harm
- Faul C, Amaral AP, Oskouei B, et al. FGF23 induces left ventricular hypertrophy. J Clin Invest. 2011;121(11):4393-4408.
- Serum phosphorus, cardiovascular and all-cause mortality in the general population: a meta-analysis. Clin Chim Acta. 2016.
Intervention: lowering phosphate additives reduces FGF23
- Impact of lowering phosphate additive intake on metabolism and cardiovascular health in community-living adults. ClinicalTrials.gov NCT02620449.
Source of the phosphate-additive prevalence figure
- Hasenböhler A, Javaux G, Payen de la Garanderie M, et al. Preservative food additives, hypertension, and cardiovascular diseases: the NutriNet-Santé study. Eur Heart J. Published online 20 May 2026. doi:10.1093/eurheartj/ehag308 PDF
Related in VitaminDWiki
- CYP27A1
- Vitamin D genes – Review
- Vitamin D Metabolite Profiling and genes (CYP24A1, CYP27B1)
- CYP27B1
- Vitamin D deficiency is associated with 35 genes, only 7 of are commercially tested
- Genes such as CYP27B1, CYP24A1 and Vitamin D – JAMA