Model has 80 percent chance of predicting vitamin D levels to within 10 ng
Determinants of plasma 25-hydroxyvitamin D and development of prediction models in three US cohorts.
Bertrand KA, Giovannucci E, Liu Y, Malspeis S, Eliassen AH, Wu K, Holmes MD, Laden F, Feskanich D.
Department of Epidemiology, Harvard School of Public Health, 677 Huntington Avenue, Boston, MA 02115, USA.
Epidemiological and other evidence suggests that vitamin D may be protective against several chronic diseases. Assessing vitamin D status in epidemiological studies, however, is challenging given finite resources and limitations of commonly used approaches.
Using multivariable linear regression, we derived predicted 25-hydroxyvitamin D (25(OH)D) scores based on known determinants of circulating 25(OH)D, including
age,
race,
UV-B radiation flux at residence,
dietary and supplementary vitamin D intakes,
BMI,
physical activity,
alcohol intake,
post-menopausal hormone use (women only) and
season of blood draw,
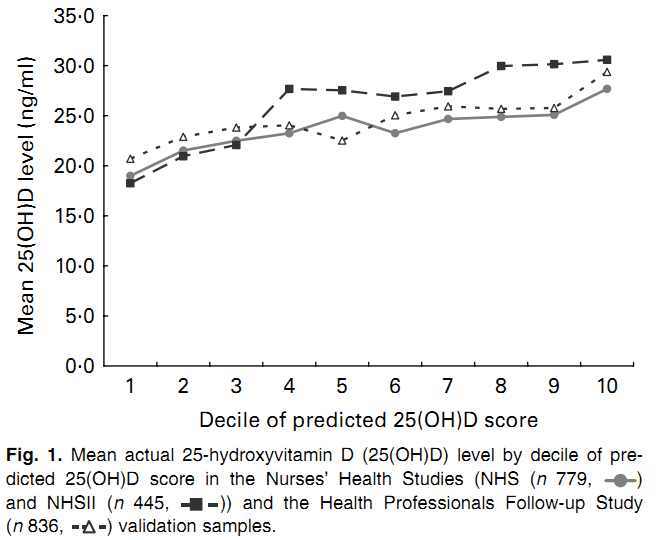
in three nationwide cohorts: the Nurses' Health Study, Nurses' Health Study II and the Health Professionals Follow-up Study.
The model r2 for each cohort ranged from 0·25 to 0·33.
We validated the prediction models in independent samples of participants from these studies.
Mean measured 25(OH)D levels rose with increasing decile of predicted 25(OH)D score, such that the differences in mean measured 25(OH)D between the extreme deciles of predicted 25(OH)D were in the range 8·7-12·3 ng/ml.
Substituting predicted 25(OH)D scores for measured 25(OH)D in a previously published case-control analysis of colorectal cancer yielded similar effect estimates with OR of approximately 0·8 for a 10 ng/ml difference in either plasma or predicted 25(OH)D.
We conclude that these data provide reasonable evidence that a predicted 25(OH)D score is an acceptable marker for ranking individuals by long-term vitamin D status and may be particularly useful in research settings where biomarkers are not available for the majority of a study population.
Note: the model covers just mid-range vitamin D levels
Best fitting model seen as of Feb 2012
They do not include many other items associated with vitamin D deficiency
from Many reasons why vitamin D deficiency has become epidemic
Air conditioning -which permits avoiding the hot sun
Work indoors vs out
Living in cities more - where there is less UV and they have less opportunity to be outdoors
Air pollution reduces UV and thus vitamin D
Fear skin cancer - so stay out of sun even in the area has a lot of UVB
Use of sun tan palors
Low Cholesterol- which the skin need to produce vitamin D
Use of Soft drink cola - uses up Calcium which uses up vitamin D
Some drugs consume vitamin D
Excessive clothing (burka, nun habit, . . .)
Have a condition or treatment which Consumes vitamin D
Have a condition which Prevents Adsorption in the gut
Have a condition which Prevents Conversion to active vitamin D: Kidney, HIV
Pregnancy
Had recent Surgery or trauma
Lactose Intolerance or Vegan – and thus not get vitamin D from milk in US and a few other countries
Health reasons to avoid sun (skin cancer, burn easily - redhead, etc) - ALTERNATIVES
Work long hours or night shift Long hours reduced vitamin D by 8% – April 2011
Exposed to DDT and some other pesticides
See also VitaminDWiki
Predicted vitamin D levels during pregnancy were sort of similar to those measured – Jan 2013
Vitamin D deficiency predicted with 80 percent accuracy with just 11 parameters – June 2013
- many of the same parameters as the study on this page
30 percent of variation of vitamin D levels were associated with just 3 variables – March 2013
Predict Vitamin D category listing has items along with related searches