Lead reduces the active form of Vitamin D (Calcitriol)
Most of this page was made by Claude AI April 2026
The lead/vitamin D relationship is well-established and bidirectional
Lead impairs vitamin D activation via CYP27B1
The classic finding (Rosen, Chesney, Mahaffey, et al., early-to-mid 1980s) is that children with elevated blood lead show reduced serum 1,25(OH)₂D even when 25(OH)D is adequate.
The mechanism is inhibition of renal CYP27B1 (1α-hydroxylase) — lead disrupts the mitochondrial cytochrome P450 system. The effect was detectable at blood lead levels that were considered "low" even by the standards of that era (≥12 µg/dL in some studies), and the dose-response was roughly linear. This is one of the cleaner demonstrations that lead toxicity includes an endocrine-disruption component, not just hematologic and neurologic effects.
Vitamin D status modulates lead absorption and distribution.
Lead hijacks calcium transport machinery — intestinal absorption via CaBP/calbindin (VDR-regulated), bone incorporation via calcium-handling proteins, and renal reabsorption. So the picture is mixed: - In calcium-deficient states, vitamin D repletion upregulates intestinal calcium absorption and also increases lead absorption if dietary lead is present. - In calcium-sufficient states, adequate vitamin D and calcium together are protective because calcium outcompetes lead at the absorption sites. - Bone is the dominant lead reservoir (~90–95% of body burden in adults). Anything that drives bone turnover — vitamin D deficiency with secondary hyperparathyroidism, pregnancy, lactation, menopause — mobilizes stored lead back into circulation. This is why maternal lead can rise during pregnancy even without new exposure, and why vitamin D adequacy that suppresses PTH is protective against endogenous lead mobilization.
VDR polymorphisms affect lead kinetics.
The Fok1 and Bsm1 VDR variants have been linked to differential blood and bone lead levels in occupationally exposed cohorts and in children (Schwartz, Onalaja, and others). The ff genotype at Fok1 and the bb at Bsm1 tend to show higher bone lead accumulation. This is mechanistically consistent with VDR's role in regulating calcium-handling proteins that lead piggybacks on.
Practical implications for VitaminDWiki framing: - Vitamin D deficiency worsens lead toxicity through at least two routes: reduced calcitriol (which lead itself suppresses, creating a feedback loop) and elevated PTH driving bone resorption of stored lead. - Repletion protocol matters. Giving vitamin D without adequate calcium in a lead-burdened population can theoretically increase absorption of ongoing dietary lead; the standard recommendation pairs them. - This is relevant to populations you're targeting. FDPIR/IHS populations have documented elevated environmental lead exposure in some regions (older housing stock, legacy soil contamination on some reservations, some traditional foods), overlapping with vitamin D deficiency. The combined insult is synergistic, not just additive.
Key older references worth anchoring on: Rosen JF et al., J Pediatr 1980; Mahaffey KR et al., NEJM 1982; Chesney RW et al., later work on calcitriol in lead-poisoned children. More recent work on VDR polymorphisms: Haynes EN et al., and several occupational cohorts from Korea and China.
Vitamin D has been observed to decrease Lead in the blood (up to 39 ng)
Short answer: yes, consistently in observational data — but the evidence base is almost entirely cross-sectional/associational, with essentially no intervention RCTs demonstrating that vitamin D supplementation reduces lead-related clinical outcomes (cognitive, behavioral, hematologic) in lead-burdened children. That's a real gap worth flagging honestly in a VitaminDWiki page.
The observational evidence is strong and recent.
A 2024 Chinese cross-sectional study of preschoolers (ages 3–6) found an L-shaped inverse relationship: each 1 ng/mL increase in vitamin D was associated with a 0.29 µg/L decrease in blood lead, with a threshold effect at around 38.7 ng/mL beyond which further reductions plateaued. The threshold finding is interesting — it's consistent with the general vitamin D sufficiency range and suggests that pushing much higher may not yield additional lead-protective benefit (at least not through this mechanism).
A 2025 Chinese study of 653 children added mechanistic detail: lower vitamin D and higher inflammatory markers in lead-exposed children, with a dose-dependent Pb → vitamin D relationship mediated by inflammatory responses. This is the inflammation-as-mediator hypothesis — lead drives chronic inflammation, which suppresses vitamin D metabolism, on top of the direct_ CYP27B1_ inhibition.
A Kuwait middle-school study reinforced the bidirectionality and proposed a clinical implication: high Pb toxicity prevalence may contribute to high VDD prevalence, so eliminating Pb sources may also improve vitamin D status. They recommended screening protocols linking the two conditions.
The Kemp/Kersey paradox is worth addressing head-on.
The 2007 Kemp et al. paper (paired winter/summer sampling in urban children) found a 32.4% winter-to-summer increase in blood lead in 1–3 year olds, and 13.0% in 4–8 year olds, roughly tracking seasonal vitamin D increases. This got interpreted two ways: (a) summer outdoor play increases environmental lead exposure (simpler explanation), or (b) rising vitamin D was actually increasing gut absorption of ongoing dietary/environmental lead — the pro-absorption concern. This is why people sometimes wrote cautionary pieces about supplementing lead-exposed kids with vitamin D.
Stephensen et al. addressed the supplementation-safety question directly in a 12-week RCT: 4000 IU/day or 7000 IU/day vitamin D3 supplementation in children and young adults with HIV did not alter blood lead concentrations. Small study, not lead-exposed at baseline, but it's the cleanest direct safety data we have against the Kemp concern.
The bone-turnover mediation story is the cleaner causal model.
A T2D study found vitamin D's association with blood lead was fully mediated by bone turnover markers, suggesting vitamin D protects against lead exposure from the bone reservoir by decreasing bone turnover. This is the mechanism I mentioned in my previous response — vitamin D adequacy suppresses PTH, which reduces osteoclastic mobilization of stored lead back into circulation. In children with active bone growth this is somewhat different, but the principle holds for pregnant women, lactating mothers, and adults with accumulated bone lead burden.
The "fewer problems" question — cognitive/developmental outcomes.
Here the direct evidence is thin. The ATSDR summary notes that lead impedes conversion of vitamin D into 1,25-dihydroxyvitamin D, which may impair cell growth, maturation, and tooth and bone development, with effects most striking in children with BLLs >62 µg/dL and chronic nutritional deficiency. So the pathway for "problems" is partly mediated through lead-induced functional vitamin D deficiency.
No study (that I found in this search) has directly tested whether vitamin D repletion in lead-exposed children improves cognitive or behavioral outcomes. The closest analog is the separate literature showing higher childhood 25(OH)D associated with better neurodevelopmental scores (Brigance, WISC) — a Medical University of South Carolina post-hoc analysis found higher 25(OH)D at time of testing associated with better overall Brigance quotient performance, and higher maternal vitamin D doses during pregnancy linked to better language scores in offspring. But that's not specifically in lead-exposed kids.
How I'd frame this on a VitaminDWiki page:
The defensible claims are:
- (1) children with higher vitamin D have consistently lower blood lead in observational studies (dozens of studies now, including recent large ones from China and Kuwait);
- (2) mechanistic pathways are plausible and multiple (CYP27B1 inhibition, bone turnover, inflammation, calcium competition at gut);
- (3) vitamin D supplementation appears safe regarding lead mobilization when calcium is adequate;
- (4) whether repletion produces measurable clinical benefit in already-exposed children is an evidence gap that needs an RCT nobody is funding — which is a recurring structural problem for vitamin D generally.
Worth considering for the page: the absence of a Mendelian randomization study using VDR polymorphisms as instruments for vitamin D status against lead outcomes. That design could partially bypass the confounding problem (SES, nutrition, housing age all co-vary with both vitamin D and lead exposure), and the data likely already exist in cohorts like NHANES — it's just a matter of somebody running it.
L-shaped relationship of Vitamin D and blood lead levels among preschool children age 3–6: A cross-sectional study
Feb 2025 https://doi.org/10.1016/j.cegh.2024.101864
CYP27B1 reduces active vitamin D (Calcitriol)
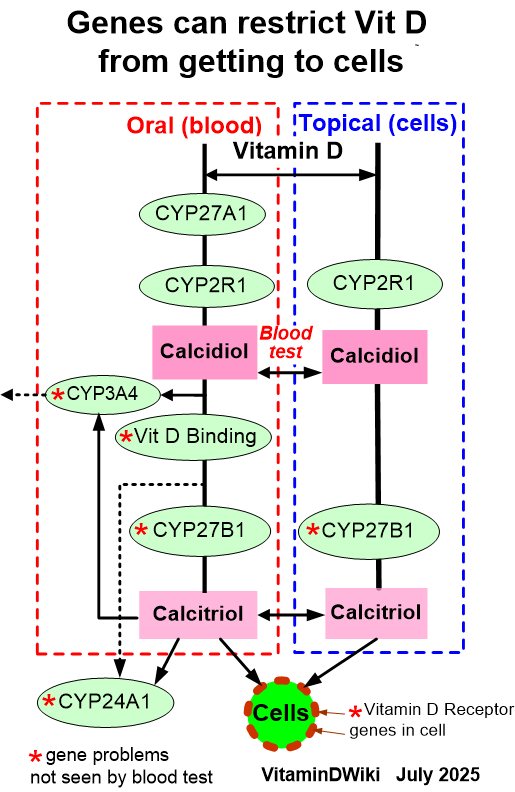
- details at: Genetics
VitaminDWiki: Lead toxicity might be reduced by Vitamin D
- "The average person today have about 625 times more lead in his system than someone of fifty years ago"
- "5.5 million annual deaths from Lead, 1 in 3 children have too much Lead - Mercola - Oct 2023"