Hypothesis: Should test for unactivated Vitamin D, not activated
Serum cholecalciferol may be a better marker of vitamin D status than 25-hydroxyvitamin D
Medical Hypotheses, Vol 111, Feb 2018, pg 61–65, https://doi.org/10.1016/j.mehy.2017.12.017
Rolf Jorde, rolf.jorde@unn.no , G. Grimnes
 click on image for details
---
1. VitaminDWiki disagrees with the need for daily dosing
1. The body has evolved to not require daily dose of vitamin D from the sun
1. The body has evolved to not require daily dose of vitamin D from diet
1. Many clinical trials have found benefit from non-daily supplementation
Intervention - non daily category listing has items along with related searches
COPD fought by Vitamin D - many studies
Respiratory infections (RTI) cut in half by 20,000 IU weekly vitamin D if initially deficient – RCT March 2015
7 improvements in lives of veterans with chronic pain with 50,000 IU vitamin D weekly – June 2012
HbA1c levels (Diabetes) reduced by monthly 50,000 IU of vitamin D – Dec 2017
Less bone loss if take 100,000 IU vitamin D monthly – RCT Nov 2017
Blood pressure reduced by monthly 100,000 IU of vitamin D in those who were deficient – RCT Oct 2017
Monthly 120,000 IU Vitamin D plus daily Calcium was great during pregnancies – RCT Sept 2017
Preeclampsia recurrence reduced 2 X by 50,000 IU of vitamin D every two weeks – RCT July 2017
click on image for details
---
1. VitaminDWiki disagrees with the need for daily dosing
1. The body has evolved to not require daily dose of vitamin D from the sun
1. The body has evolved to not require daily dose of vitamin D from diet
1. Many clinical trials have found benefit from non-daily supplementation
Intervention - non daily category listing has items along with related searches
COPD fought by Vitamin D - many studies
Respiratory infections (RTI) cut in half by 20,000 IU weekly vitamin D if initially deficient – RCT March 2015
7 improvements in lives of veterans with chronic pain with 50,000 IU vitamin D weekly – June 2012
HbA1c levels (Diabetes) reduced by monthly 50,000 IU of vitamin D – Dec 2017
Less bone loss if take 100,000 IU vitamin D monthly – RCT Nov 2017
Blood pressure reduced by monthly 100,000 IU of vitamin D in those who were deficient – RCT Oct 2017
Monthly 120,000 IU Vitamin D plus daily Calcium was great during pregnancies – RCT Sept 2017
Preeclampsia recurrence reduced 2 X by 50,000 IU of vitamin D every two weeks – RCT July 2017
📄 Download the Sci-Hub PDF via VitaminDWiki
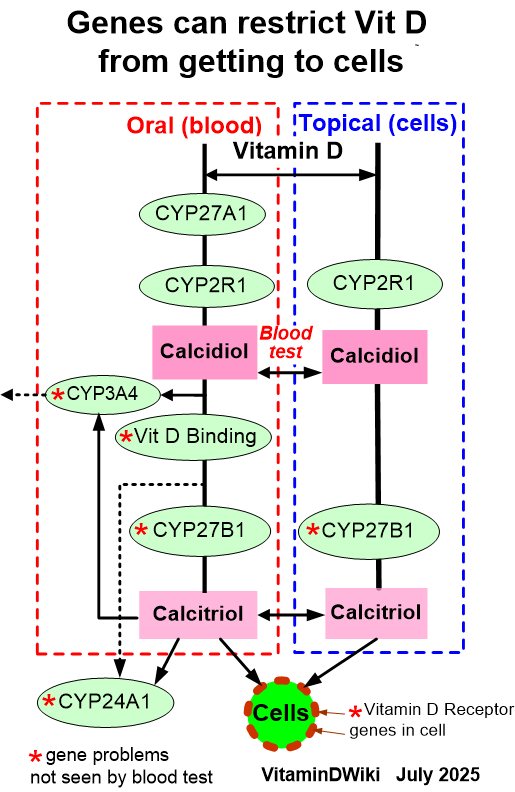
Vitamin D is produced in the skin upon sun-exposure or obtained through the diet. Vitamin D is hydroxylated to 25-hydroxyvitamin D (25(OH)D) in the liver and to the active form 1,25-dihydroxyvitamin D (1,25(OH)2D) in the kidneys. To exert its effect 1,25(OH)2D has to bind to the nuclear vitamin D receptor VDR. Lack of vitamin D leads to rickets in children and to osteomalacia in adults. 25(OH)D is used as a marker of a subject’s vitamin D status. Low serum 25(OH)D levels are associated with a number of diseases, risk factors for disease and increased mortality.
However, intervention studies with vitamin D have generally been disappointing. Many, if not most cells have the hydroxylases necessary for intra-cellular activation of vitamin D .
It is likely that more vitamin D diffuses or are transported into the cells than 25(OH)D and 1,25(OH)2D, and accordingly, most of the 1,25(OH)2D that bind to the VDR are derived from intra-cellular hydroxylation of vitamin D. Therefore, our hypothesis is that serum vitamin D is a better marker of a subject’s vitamin D status than 25(OH)D. Since the half-life in serum for vitamin D is approximately one day, giving vitamin D weekly or monthly will result in short-lived serum vitamin D peaks with periods of vitamin D deficiency in between. On the other hand, serum 25(OH)D, which has a half-life of weeks, will show high and stable serum levels throughout.
Important vitamin D effects may have been missed in studies with intermittent dosing, and vitamin D in intervention trials should be given daily .
Likewise, in epidemiological studies and clinical practice 25(OH)D has uniformly been used as marker. This may lead to gross misclassification of individuals that do not have a stable influx of vitamin D from sun-exposure or diet. In epidemiological studies serum vitamin D should be measured as well as 25(OH)D, and in clinical practice a 25(OH)D measurement should be interpreted in view of recent sun-exposure and diet history.
Clipped from PDF
Thus, in the circulation six main forms (or complexes) are found:
free vitamin D
DBP-bound vitamin D
free 25(OH)D
DBP-bound 25(OH)D
free 1,25(OH)2D
DBP-bound 1,25(OH)2D
Assumptions:
large quantities of circulating unbound vitamin D easily diffuse across cell membranes
CYP2R1 and other yet unidentified 25-hydroxylases are widely distributed
the activity of CYP2R1 in peripheral tissues is likely to be unrestricted as in the liver
the megalin/cubulin system will provide both vitamin D and 25(OH)D into the cells
Monthly vs daily dose
In a study by Oberhelman et al. lactating women were randomized to 150 000 IU once or 5000 IU daily for 28 days. At the end of the trial both groups had mean serum 25(OH)D slightly above 100 nmol/L, whereas in the bolus dose group mean serum vitamin D was 17.5 nmol/L versus 45.8 nmol/L in the daily dose group (30).